Резюме
Актуальність. Харчування є однією з найважливіших причин появи каменів у нирках. Це дослідження було розроблено для оцінки літогенних факторів у раціоні пацієнтів із нефролітіазом. Матеріали і методи. У дослідження ввійшли 40 пацієнтів із сечокам’яною хворобою, які не мали метаболічних порушень, що приводили б до утворення каменів (таких як гіперпаратиреоз, первинна гіпероксалурія). Проводились оцінка антропометричних даних (індекс маси тіла, співвідношення окружностей талії та стегон), аналіз композиційного складу тіла (біоімпедансний аналіз складу тіла), якісний і кількісний аналіз харчових звичок пацієнтів (3-денна реєстрація їжі, що приймається). Результати. У половини пацієнтів відмічались надлишкова вага або ожиріння. Їх раціон містив велику кількість білка, жиру, фосфору, вітаміну С й невелику кількість рідини, кальцію, магнію, калію, вітаміну В6. Споживання білка позитивно корелювало із споживанням сечової кислоти (r = 0,78), а маса тіла — із рівнем жиру в раціоні (r = 0,58) і споживанням сечової кислоти (r = 0,55). Висновки. Повний курс лікування із приводу нефролітіазу повинен включати дієтотерапію. Відсутність змін у звичайному раціоні пацієнтів із сечокам’яною хворобою може стимулювати процес літогенезу.
Актуальность. Питание является одной из важнейших причин появления камней в почках. Это исследование было разработано для оценки литогенных факторов в рационе пациентов с нефролитиазом. Материалы и методы. В исследование вошли 40 пациентов с мочекаменной болезнью, не имеющих метаболических нарушений, которые приводили бы к образованию камней (таких как гиперпаратиреоз, первичная гипероксалурия). Проводились оценка антропометрических данных (индекс массы тела, соотношение окружностей талии и бедер), анализ композиционного состава тела (биоимпедансный анализ состава тела), качественный и количественный анализ пищевых привычек пациентов (3-дневная регистрация принимаемой пищи). Результаты. У половины пациентов отмечались избыточный вес или ожирение. Их рацион содержал большое количество белка, жира, фосфора, витамина С и небольшое количество жидкости, кальция, магния, калия, витамина В6. Потребление белка положительно коррелировало с потреблением мочевой кислоты (r = 0,78), а масса тела — с уровнем жира в рационе (r = 0,58) и потреблением мочевой кислоты (r = 0,55). Выводы. Полный курс лечения по поводу нефролитиаза должен включать в себя диетотерапию. Отсутствие изменений в обычном рационе пациентов с мочекаменной болезнью может стимулировать процесс литогенеза.
Background. Nutrition is one of the most important determinants of kidney stone formation. This study was designed to evaluate lithogenic factors in diet of patients with renal calculi. Materials and methods. 40 stone-formers without metabolic disorders stimulating stone formation (e.g. hyperparatyroidism, primary hyperoxaluria) were invited to the study. Antropometric measurements of nutritional status (BMI, WHR), analysis of body composition (BIA), quality and quantitative analysis of patients’ eating habits (3-day food records) were conducted. Results. Half of patients were overweight or obese. Their diets contained high amounts of protein, fat, phosphorus, vitamin C and low amounts of fluid, calcium, magnesium, potassium, vitamin B6. Protein consumption was positively correlated with uric acid intake in diets (r = 0.78), and body weight with dietary fat intake (r = 0.58) and uric acid intake (r = 0.55). Conclusions. Complete treatment of nephrolithiasis should include nutritional therapy. No change in customary diets of patients with renal calculi can stimulate lithogenesis process.
Introduction
Kidney stone (renal calculus, lat. nephrolithasis, urolithasis) is the third most frequent urinary disease. It occurs on the entire world and affects up to 5 % of the population between 30 and 50 years old which indicates that the disease is a serious social issue in industrialized countries prevalence of nephrolithiasis ranges from 1 to 10 %. Most kidney stones are composed of calcium salts (oxalate, phosphate) [1, 2]. The main causes of stone formation are genetic and environmental factors. Fa–mily history of kidney calculi enhances its incidence [3]. Some scientists called nephrolithiasis a “nutritional di–sease”. A significant role in ethiology of the disease is a diet. Diets rich in fat (indirectly) and animal protein (directly) stimulate lithogenesis [4]. In our study we tried to find basic nutritional factors among patients with kidney stones, which may be lithogenic factors.
Materials and methods
We invited patients with kidney stones from Kolejowy Central Hospital, Baby Jesus Hospital Nephrological-Transplant Clinic and Individual Specialistic Medical Practice in Urology Clinic in Gdansk treating patients with urinary tract diseases, including kidney stone, to take part in the study.
The exclusion criteria were hyperparatyroidism, primary hyperoxaluria or other metabolic disorders stimulating stone formation. 42 patients gave their assent to participate in the study. None of them received any specific dietary consultation before the study. Glomural filtration rate was estimated on the basis of Levey et al. formula [5]. Body Mass Index (BMI) and Waist-Hips Ratio (WHR) were calculated as weight (kg) divided by height squared (m2) and waistline (cm) divided by hips line (m), adequately. Bioimpedance was done according to standardised procedures [6]. In this analysis we used 3-day food records and also on their basis we specified energy and other nutrients intake by means of a computer software Dietetyk, based on Polish Food Nutrition Tables [7]. The results are presented as mean ± SD. BMI, energy, n3, n3/n6 and fibre intakes, because the lack of normal distribution is presented as the median. Since the study was conducted before 2008 the results referred to dietary guidelines for Poland of that time [8].To describe differences between men and women we used Student’s test and nonparametric Mann-Whitney test (STATGRAPHICS Plus 4.0). To evaluate correlation simple linear regression analysis was applied.
Results
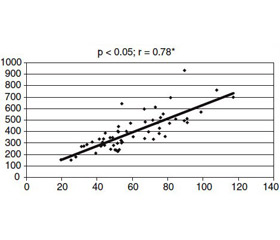
The characteristics of 42 stone formers are presented in Table 1. There was not any difference in the age of patients, but men had higher BMI and WHR. Among 28 participants with long history of nephrolithiasis (more than 3 years) occurred episodes of recurrence of kidney stones. The most common components of calculi were oxalate salts. A family history of kidney stones occurred with 24 patients. The efficiency of kidney measured by glomular filtration rate indicated mainly not significant kidney’s impairment. Only in two women kidney stones essentially damaged renal function (Table 2). Men had higher and statistically significant BMI and WHR para–meters (Table 1), compared with women. The waistlines of 50 % men were more than 102 cm. Bioelectrical Impedance Analysis test was performed on 42 patients with kidney stones. Only 7 participants had normal percen–tage of body fat but the total body water, as an estimate of hydration level, was insufficient in 35 persons. Results of quantitative analysis menu patients with nephrolithiasis are summarized in Table 3. Dietary energy intake in group of men was significantly higher than in the group of women which resulted from high intake of protein and fat in men’s diets. Men also drank more fluids on a daily basis, compared with women, but in both groups this value was lower than recommended (more than 2.5 L per day) [9]. We did not find any correlation between total fluid intake and total body water intake. Meat products eaten every day were the main source of protein in diets. We observed positive correlation between dietary total protein intake and uric acid intake as well (Fig. 1) although body weight of patients was correlated with dietary fat intake (Fig. 2) and uric acid intake (Fig. 3). Furthermore, inconsiderable correlation was found between dietary fat intake and body fat mass (p = 0.0506, r = 0.51).
/47-1.jpg)
/48-1.jpg)
/49-1.jpg)
Discussion
The first episode of nephrolithiasis may appear even in childhood triggered by primary hiperoxaluria [10, 11] and in our study age range of patients with kidney stones was wide (23–76 years). Recurrent renal stone disease is very frequent and occurs in about 50 % stone formers [13]. In most participants of the study stones recurred too and the most common type was oxalate salts just like in other studies [10, 14]. A family history of kidney stones enhanced the risk of development of the disease in individuals. Curhan et al. [13] in a cohort the Health Professionals Follow-up Study of 37 999 men showed that in male stone formers a family history of nephrolithiasis was more common than in those without kidney stones. Our study indicated the same relation. Long-term stone formation with recurrences may increase the risk of chronic kidney failure leading to glomerulosclerosis and decreased glomular filtration rate by obstruct calyces and renal pelvis [15]. Two women in this study had very low GFR, which indicated almost end-stage renal di–sease. Overweight and obesity may stimulate renal stones formation. Positive correlations between body weight, BMI and nephrolithiasis can be found in many studies [16, 17]. Maalouf et al. [18] and Abate et al. [19] revealed that excess percentage body fat and insulin resistance lower pH in urine enhance the risk of uric acid kidney stones. In our study most patients had quite high value of BMI, WHR (particularly men) and body fat (particularly women). Diets of patients with kidney stones supplied low intakes of fluids, fibre and high intakes of protein, fat, especially in a group of men. Diets with insufficient participation of fluid stimulate salts crystallisation in urine and stone formation [20]. In this group additional lithegenic factor was type of beverages (first of all black tea and coffee), as we mentined in Roczn PZH [21]. Excess animal protein in our studyand positive correlation with dietary uric acid intake may acidify urine and cause hypercalciuria [19–22]. Giannini et al. [23] showed that 0.8 g protein/kg/day significantly reduced serum and urinary urea values, similarly like urinary calcium and oxalate. Vegetarian diets, compared to the westerntype diets, decrease the risk of uric acid crystallisation by 93 % [24]. But Massey and Kynast-Gales [25] revealed a more important relationship between protein intake than the type of protein. Positive correlation between body weight of patients with kidney stones and fat intake implies that it could be the main cause of overweight and obesity and high percen–tage body fat among the participants. Additionally, higher uric acid consumption among patients with higher body weight can undoubtedly stimulate stone formation. On the other hand, fibre may protect from nephrolithiasis. Hess et al. [26] proved that fibre enhances urinary citrate excretion which dissolves calcium oxalate salts. However, in diets of our patients this nutrient was in insufficient intake as well, which indicates low consumption of fruit and vegetables. Low potassium and magnesium intake may stimulate stone formation by reduced reabsorption of calcium in tubule and decreased concentration of natural inhibitor of crystallisation of calcium oxalate, which is magnesium. Furthermore, among other nutritional lithogenic factors, which have been described by us in Roczn PZH [21], we can rate low diet intake of calcium, vitamin B6 and high intake of oxalic acid, vitamin C.
Conclusions
Nutrition can stimulate lithogenesis. Patients with kidney stones should have an opportunity to talk to dietitians about their nutritional habits and receive accurate dietetic recommendations.
Conflicts of interests. Authors declare the absence of any conflicts of interests that might be construed to influence the results or interpretation of their manuscript.
Reviewers: N. Zheltovska, PhD, Senior Research Fellow at the State institution “Institute of urology of the Ministry of Health of Ukraine” and Dmytro D. Ivanov, MD, PhD, Professor, Head of the Department of nephrology and renal replacement therapy, Shupyk National Medical Academy of Postgraduate Education
Список литературы
1. Pak CY. Kidney stones. Lancet. 1998 Jun 13;351(9118):1797-801. doi: 10.1016/S0140-6736(98)01295-1.
2. Bihl G, Meyers A. Recurrent renal stones disease-advances in pathogenesis and clinical management. Lancet. 2001 Aug 25;358(9282):651-6. doi: 10.1016/S0140-6736(01)05782-8.
3. Roudakova K, Monga M. The evolving epidemiology of stone disease. Indian J Urol. 2014 Jan-Mar;30(1):44-8. doi: 10.4103/0970-1591.124206.
4. Han H, Segal AM, Seifter JL, Dwyer JT. Nutritional Management of Kidney Stones (Nephrolithiasis). Clin Nutr Res. 2015 Jul;4(3):137-52. doi: 10.7762/cnr.2015.4.3.137.
5. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999 Mar 16;130(6):461-70. PMID: 10075613.
6. Oldham NM. Overview of bioelectrical impedance analyzers. Am J Clin Nutr. 1996 Sep;64(3 Suppl):405S-412S. PMID: 8780356.
7. Kunachowicz H, Nadolna I, Przygoda B, Iwanow K. Food Composition Tables. Warsaw: PZWL; 2005. (in Polish).
8. Ziemlański Ś. Normy żywieniowe człowieka. Fizjologiczne podstawy [Human nutritional standards. Physiological basis]. Warsaw: PZWL; 2001. 531 p. (in Polish).
9. Cheungpasitporn W, Rossetti S, Friend K, Erickson SB, Lieske JC. Treatment Effect, Adherence, and Safety of High Fluid Intake for the Prevention of Incident and Recurrent Kidney Stones: a Systematic Review and Meta-Analysis. J Nephrol. 2016 Apr;29(2):211-19. doi: 10.1007/s40620-015-0210-4.
10. Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol. 2000 Nov-Dec;13 Suppl 3:S45-50. PMID: 11132032.
11. Alatab S, Pourmand G, El Howairis Mel F, et al. National Profiles of Urinary Calculi: a Comparison Between Developing and Developed Worlds. Iran J Kidney Dis. 2016 Mar;10(2):51-61. PMID: 26921745.
12. Curhan GC, Willett WC, Rimm EB, Speizer FE, Stampfer MJ. Body size and risk of kidney stones. J Am Soc Nephrol. 1998 Sep;9(9):1645-52. PMID: 9727373.
13. Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Family history and risk of kidney stones. J Am Soc Nephrol. 1997 Oct;8(10):1568-73. PMID: 9335385.
14. Tuma J, Hess B. Nephrolithiasis: Epidemiologie, Pathophysiologie, Vorgehen bei Nierenkolik, bildgebende Diagnostik. Swiss Med Forum. 2001;01(41):1019-24. doi: 10.4414/smf.2001.04303. (in German).
15. Vupputuri S, Soucie JM, McClellan W, Sandler DP. History of kidney stones as a possible risk factor for chronic kidney disease. Ann Epidemiol. 2004 Mar;14(3):222-8. doi: 10.1016/S1047-2797(03)00126-1.
16. Siener R, Glatz S, Nicolay C, Hesse A. The role of overweight and obesity in calcium oxalate stone formation. Obes Res. 2004 Jan;12(1):106-13. doi: 10.1038/oby.2004.14.
17. Lemann J Jr, Pleuss JA, Worcester EM, Hornick L, Schrab D, Hoffmann RG. Urinary oxalate excrection increases with body size and decreases with increasing dietary calcium intake among healthy adults. Kidney Int. 1996 Jan;49(1):200-8. PMID: 8770968.
18. Maalouf NM, Sakhaee K, Parks JH, Coe FL, Adams-Huet B, Pak CY. Association of urinary pH with body weight in nephrolithiasis. Kidney Int. 2004 Apr;65(4):1422-5. doi: 10.1111/j.1523-1755.2004.00522.x.
19. Abate N, Chandalia M, Cabo-Chan AV Jr, Moe OW, Sakhaee K. The metabolic syndrom and uric acid nephrolithiasis: Novel features of renal manifestation of insulin resistance. Kidney Int. 2004 Feb;65(2):386-92. doi: 10.1111/j.1523-1755.2004.00386.x.
20. Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol. 1996 Mar;155(3):839-43. PMID: 8583588.
21. Gasińska A, Gajewska D. Tea and cofee as the main sources of oxalate in diets patients with kidney oxalate stones. Rocz Panstw Zakl Hig. 2007;58(1):61-7. PMID: 17711092.
22. Hess B, Casez JP, Takkinen R, Ackermann D, Jaeger P. Relative hypoparathyroidism and calcitriol up-regulation in hypercalciuric calcium renal stone formers-impact of nutrition. Am J Nephrol. 1993;13(1):18-26. PMID: 8322837.
23. Giannini S, Nobile M, Sartori L, et al. Acute effects of moderate dietary protein restriction in patients with idiopathic hyperkalciuria and calcium nephrolithiasis. Am J Clin Nutr. 1999 Feb;69(2):267-71. PMID: 9989691.
24. Siener R, Hesse A. The effect of a vegetarian and different omnivorous diets on urinary risk factors for uric acid stone formation. Eur J Nutr. 2003 Dec;42(6):332-7. doi: 10.1007/s00394-003-0428-0.
25. Massey LK, Kynast-Gales SA. Diets with either beef or plant proteins reduce risk of calcium oxalate precipitation in patients with a history of calcium kidney stones. J Am Diet Assoc. 2001 Mar;101(3):326-31. doi: 10.1016/S0002-8223(01)00085-2.
26. Hess B, Michel R, Takkinen R, Ackermann D, Jaeger P. Risk factors for low urinary citrate in calcium nephrolithiasis: low vegetable fibre intake and low urine volume to be added to the list. Nephrol Dial Transplant. 1994;9(6):642-9. PMID: 7970090.

/47-1.jpg)
/48-1.jpg)
/49-1.jpg)