Резюме
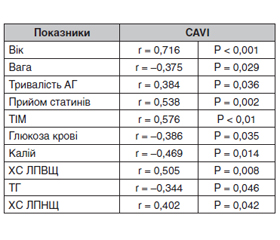
Метою цього дослідження була оцінка артеріальної жорсткості, яка змінилася після додавання статинів до фіксованої комбінованої антигіпертензивної терапії в пацієнтів з резистентною артеріальною гіпертензією. Матеріали та методи. Включено 99 хворих на помірну й тяжку артеріальну гіпертензію без цукрового діабету. Ці пацієнти були розподілені на 2 групи. Першій групі (n = 59) було призначено фіксовану комбінацію антигіпертензивної терапії плюс аторвастатин 20–40 мг/добу. Пацієнти другої групи (n = 40) отримували фіксовану комбінацію антигіпертензивних препаратів без статинів. Серцево-гомілковий судинний індекс (CAVI) визначався до і в кінці періоду спостереження. Проводилися моніторинг офісного артеріального тиску (АТ), добове моніторування артеріального тиску (ДМАТ). Були проведені лабораторні дослідження: загальний аналіз крові, аналіз сечі та біохімічний аналіз крові. Тривалість дослідження становила 6 місяців. Результати. Офісний АТ і показник ДМАТ однаково значно знизилися в обох групах лікування. Рівні загального холестерину (ЗХС) і холестерину ліпопротеїдів низької щільності (ХС ЛПНЩ) значно знизилися в групі аторвастатину на 1,76 ммоль/л (30 %, р < 0,05) і 1,51 ммоль/л (41 %, р < 0,05) відповідно. У групі без терапії аторвастатином не було змін рівня ЗХС і ХС ЛПНЩ. У групі без додавання статинів відзначено достовірне зниження рівня АТ, однак CAVI підвищився до +0,9 од. справа та +1,0 од. зліва. У групі без додавання статинів CAVI після лікування змінився з 7,73 ± 0,17/7,62 ± 0,19 од. до 8,63 ± 0,22/8,62 ± 0,12 од. справа/зліва відповідно (p < 0,05). Це означає, що в групі без додавання статинів через 6 місяців терапії спостерігалося збільшення жорсткості артеріальної стінки за CAVI. У групі з додаванням статину після 6 місяців терапії CAVI не змінився: CAVI справа/зліва становив 8,32 ± 0,16/8,33 ± 0,19 од. на початку і 8,44 ± 0,16/8,24 ± 0,15 од. — після лікування (p > 0,05). Впливу статинотерапії на рівень АТ ми не відзначили. Проте було виявлено кореляційні зв’язки між CAVI та віком, рівнем тригліцеридів до лікування, ХС ЛПНЩ, тривалістю гіпертензії, рівнем глюкози в крові. Висновки. Додавання аторвастатину до фіксованої комбінації антигіпертензивної терапії може запобігти прогресуванню жорсткості артерій у пацієнтів з артеріальною гіпертензією.
Background. The purpose of this study was to evaluate the arterial stiffness, which changed after adding statins to a fixed-dose combination antihypertensive therapy in patients with resistant hypertension. Materials and methods. The study included 99 patients with moderate and severe hypertension without diabetes. They were divided into 2 groups. The first group (n = 59) took a fixed-dose combination antihypertensive therapy plus atorvastatin 20–40 mg/day. Patients in the second group (n = 40) received a fixed-dose combination antihypertensive treatment without statins. The cardio-ankle vascular index (CAVI) was evaluated before treatment and at the end of the follow-up. Furthermore, the office blood pressure (BP) monitoring was performed, as well as the ambulatory blood pressure monitoring (ABPM). The laboratory studies also took place such as the complete blood count, urinalysis and blood biochemistry tests. The study duration was 6 months. Results. Office BP and ABPM had decreased significantly and equally in both treatment groups. Total cholesterol and low-density lipoprotein (LDL) cholesterol had decreased significantly in the atorvastatin group, by 1.76 mmol/l (30 %, p < 0.05) and 1.51 mmol/l (41 %, p < 0.05), respectively. In the group without atorvastatin therapy, there were no changes in the level of total cholesterol and LDL cholesterol. In the group without statins, a significant decrease in the level of BP was noted; however, the CAVI increased to +0.9 units on the right side and +1.0 units on the left side. In the group without statin addition, the CAVI changed from 7.73 ± ± 0.17/7.62 ± 0.19 units to 8.63 ± 0.22/8.62 ± 0.12 units on the right/left side after treatment (p < 0.05). It means that there was an increase in the arterial stiffness in terms of the CAVI in the group without statins after 6 months of therapy. In the group with statin addition, the CAVI did not change after 6 months of therapy: on the right/left side, it was 8.32 ± 0.16/8.33 ± 0.19 units at baseline and 8.44 ± 0.16/8.24 ± 0.15 units (p > 0.05) after treatment. We did not note any impact of statin therapy on the BP level. However, a significant correlation was found between the CAVI and age, serum level of triglycerides before treatment, LDL cholesterol, duration of hypertension, the blood glucose level. Conclusions. Adding atorvastatin to a fixed-dose combination antihypertensive therapy could prevent the progression of arterial stiffness in patients with hypertension.
Список литературы
1. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002. Vol. 18. 288(23). P. 2981-2997. DOI:10.1001/jama.288.23.2998.
2. Aranda P., Ruilope L.M., Calvo C., Luque M., Coca A., de Miguel A.G. Erectile dysfunction in essential arterial hypertension and effects of sildenafil: results of a Spanish national study. Am. J. Hypertens. 2004. Vol. 17(2). P. 139-145. DOI: 10.1016/j.amjhyper.2003.09.006.
3. Bukuda К., Ichihara A., Sakoda M., Mito A., Kinouchi K., Itoh H. Blood pressure-independent effect of candesartan on cardio-ankle vascular index in hypertensive patients with metabolic syndrome. Vasc. Health Risk Manag. 2010. 6. 571-578. DOI:10.2147/vhrm.s11958.
4. Calhoun D.A., Lacourciere Y., Crikelair N., Jia Y., Gla–zer R.D. Effects of demographics on the antihypertensive efficacy of triple therapy with amlodipine, valsartan, and hydrochlorothiazide for moderate to severe hypertension. Curr. Med. Res. Opin. 2013. Vol. 29. P. 901-910. doi: 10.1185/03007995.2013.803057.
5. Choi S.Y., Oh B.H., Park J.B., Choi D.J., Rhee M.Y., Park S. Age-associated increase in arterial stiffness measured according to the cardio-ankle vascular index without blood pressure changes in healthy adults. J. Atheroscler. Thromb. 2013. 20. 911-923. DOI: 10.5551/jat.18267.
6. Doumas M., Tsakiris A., Douma S. Grigorakis A., Papadopoulos A., Hounta A. et al. Factors affecting the increased prevalence of erectile dysfunction in Greek hypertensive compared with normotensive subjects. J. Androl. 2006. Vol. 27(3). P. 469-477. DOI: 10.2164/jandrol.04191.
7. Aydın Е., Kant А., Yilmaz G. Evaluation of the cardio-ankle vascular index in COVID-19 patients. Rev. Assoc. Med. Bras. 1992. 2022 Jan. 68(1). 73-76. doi: 10.1590/1806-9282.20210781.
8. Grant E.G., Benson C.B., Moneta G.L., Alexandrov A.V., Baker J.D., Bluth E.I. et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis — Society of Radiologists in Ultrasound Consensus Conference. Radiology. 2003 Nov. 229(2). 340-6. doi: 10.1148/radiol.2292030516.
9. Greenstein A., Chen J., Miller H., Matzkin H., Villa Y., Braf Z. Does severity of ischemic coronary disease correlate with erectile function? Int. J. Impot. Res. 1997. Vol. 9(3). P. 123-126. DOI:10.1038/sj.ijir.3900282
10. Horinaka S., Yabe A., Yagi H., Yagi H., Ishimura K., Hara H., Iemua T. Comparison of atherosclerotic indicators between cardio ankle vascular index and brachial ankle pulse wave velocity. Angiology. 2009. 60(4). 468-476. https://doi.org/10.1177/0003319708325443.
11. Ibata J., Sasaki H., Kakimoto T., Matsuno S., Nakatani M., Kobayashi M. et al. Cardio-ankle vascular index measures arterial wall stiffness independent of blood pressure. Diabetes Res. Clin. Pract. 2008. 80(2). 265-270. https://doi.org/10.1016/j.diabres.2007.12.016.
12. Kokubo Y., Watanabe M., Higashiyama A., Nakao Y.M., Nakamura F., Miyamoto Y. Impact of intima-media thickness progression in the common carotid arteries on the risk of incident cardiovascular disease in the suita study. J. Am. Heart Assoc. 2018. 7(11). e007720.
13. Mehlum M., Liestøl K., Julius S., Kjeldsen S.E., Hua T.A., Rothwell P.M. et al. Visit-to-visit blood pressure variability increases risk of stroke or cardiac events in patients given valsartan or amlodipine in the VALUE trial. J. Hypertens. 2015. Vol. 33. Suppl. 1. e40. doi: 10.1097/01.hjh.0000467454.55397.ea.
14. Miyashita Y., Endo K., Saiki A., Ban N., Yamaguchi T., Kawana H. et al. Effects of pitavastatin, a 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitor, on cardio-ankle vascular index in type 2 diabetic patients. J. Atheroscler. Thromb. 2009. 16. 539-545. https://doi.org/10.5551/jat.281.
15. Miyashita Y., Saiki A., Endo K., Ban N., Yamaguchi T., Kawana H. et al. Effects of olmesartan, an angiotensin II receptor blocker, and amlodipine, a calcium channel blocker, on Cardio-Ankle Vascular Index (CAVI) in type 2 diabetic patients with hypertension. J. Atheroscler. Thromb. 2009. 16. 621-626. DOI: 10.5551/jat.497.
16. Nakayama K., Kuwabara Y., Daimon M., Shindo S., Fujita M., Narumi H. et al. Valsartan Amlodipine Randomized Trial (VART): design, methods, and preliminary results. Hypertens. Res. 2008. Vol. 31(1). P. 21-28. doi: 10.1291/hypres.31.21.
17. Namekata T., Suzuki K., Ishizuka N., Shirai K. Establishing baseline criteria of cardio-ankle vascular index as a new indicator of arteriosclerosis: a cross-sectional study. BMC Cardiovasc. Disord. 2011. 11. 51. doi: 10.1186/1471-2261-11-51.
18. Saiki A., Sato Y., Watanabe R., Watanabe Y., Imamura H., Yamaguchi T. et al. The Role of a Novel Arterial Stiffness Parameter, Cardio-Ankle Vascular Index (CAVI), as a Surrogate Marker for Cardiovascular Diseases. J. Atheroscler. Thromb. 2016. 23(2). 155-68. doi: 10.5551/jat.32797.
19. Satoh N., Shimatsu A., Kato Y., Araki R., Koyama K., Okajima T. et al. Evaluation of the cardio-ankle vascular index, a new indicator of arterial stiffness independent of blood pressure, in obesity and metabolic syndrome. Hypertens. Res. 2008 Oct. 31(10). 1921-30. doi: 10.1291/hypres.31.1921.
20. Sawada T., Yamada H., Dahlf B., Matsubara H., for the KYOTO HEART Study Group. Effects of valsartan on morbidity and mortality in uncontrolled hypertensive patients with high cardiovascular risks: KYOTO HEART Study. Eur. Heart J. 2009. Vol. 30. P. 2461-2469. doi: 10.1093/eurheartj/ehp363.
21. Shirai K., Utino J., Otsuka K., Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J. Atheroscler. Thromb. 2006. 13(2). 101-107. doi: 10.5551/jat.13.101.
22. Shirai K., Song M., Suzuki J., Kurosu T., Oyama T., Nagayama D. et al. Contradictory effects of β1- and α1-aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI) — CAVI independent of blood pressure. J. Atheroscler. Thromb. 2011. 18(1). 49-55. DOI: 10.5551/jat.3582.
23. Sison J., Ríos Vega R.M., Dayi H., Bader G., Brunel P. Efficacy and effectiveness of valsartan/amlodipine and valsartan/amlodipine/hydrochlorothiazide in hypertension: randomized-controlled versus observational studies. Current Medical Research and Opinion. DOI: 10.1080/03007995.2017.1412682.
24. Takaki A., Ogawa H., Wakeyama T., Iwami T., Kimura M., Hadano Y. et al. Cardio-ankle vascular index is superior to brachial-ankle pulse wave velocity as an index of arterial stiffness. Hypertens. Res. 2008 Jul. 31(7). 1347-55. doi: 10.1291/hypres.31.1347.
25. Uehara G., Takeda H. Relative effects of telmisartan, candesartan and losartan on alleviateing arterial stiffnes inpatients with hypertension complicated by diabetes mellitus: An evaluation using the cardiovascular index. J. Inter. Medical Res. 2008. 36. 1094-1102. doi: 10.1177/147323000803600529.
26. Wang L., Zhao J.W., Liu B., Shi D., Zou Z., Shi X.Y. Antihypertensive effects of olmesartan compared with other angiotensin receptor blockers: a meta-analysis. Am. J. Cardiovasc. Drugs. 2012. 12(5). P. 335-344. doi: 10.2165/11597390-000000000-00000.
27. Williams B., Mancia G., Spiering W., Agabiti Rosei E., Azizi M., Burnier M. et al; Authors/Task Force Members: 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018. 36. 1953-2041. doi: 10.1097/HJH.0000000000001940.
28. Yamamoto N., Yamanaka G., Ishikawa M., Takasugi E., Murakami S., Yamanaka T. et al. Cardio-ankle vascular index as a predictor of cognitive impairment in community-dwelling elderly people: four-year follow-up. Dement. Geriatr. Cogn. Disord. 2009. 28(2). 153-158. doi: 10.1159/000235642.