
Журнал «Почки» Том 14, №1, 2025
Вернуться к номеру
Результати гемодіалізу, пов’язані із транспозицією медіальної підшкірної вени руки або синтетичним судинним протезуванням: одноцентрове дослідження
Авторы: A.M. Fahad (1), H.N. Naser (1), L.F.F. Sharba (2), H.S.K. Al-Shakarchi (1), Z.A. Yasser (1), A.A. Abed (1)
(1) - Najaf Health Directorate, Najaf, Iraq
(2) - Jabir Ibn Hayyan Medical University, Najaf, Iraq
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
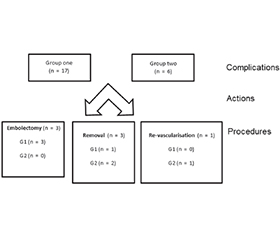
Актуальність. Для гемодіалізу кращим типом судинного доступу є автогенна радіоцефальна або брахіоцефальна фістула, тоді як фістула при транспозиції медіальної підшкірної вени руки (ТМПВР) і подальше використання протезного шунта пропонують, якщо присутні невідповідні вени. Мета: порівняти результат використання ТМПВР та синтетичного судинного протеза для діалізу в одному центрі. Матеріали та методи. У цьому дослідженні взяли участь 148 пацієнтів, розділені на дві групи: першу (n = 127; 69 чоловіків і 58 жінок, середній вік 49 років), у якій використано ТМПВР, і другу (n = 21; 15 чоловіків та 6 жінок, середній вік 58 років), пацієнтів якої прооперовано із застосовуванням синтетичного судинного протеза. Результати. Семи пацієнтам із гематомою проведено ревізію протягом 7 днів після операції (p = 0,001). Венозну гіпертензію діагностовано в трьох пацієнтів першої групи, у другій групі її не було (p = 0,001). У першій групі частота ускладнень становила 13,38 %, тоді як у другій — 28,57 % зі статистично значущою різницею (p = 0,001). У першій групі первинну прохідність зареєстровано в 96,85 % випадків проти 90,47 % у другій групі (p = 0,07). Частота асистованої первинної прохідності в першій групі дорівнювала 75 %, у другій — 0 % (p = 0,001). Висновки. Дослідження показало, що використання для гемодіалізу синтетичного протеза викликає більше ускладнень, як-от частота тромбозів, синдром ішемічного обкрадання та інфекції, ніж доступ через медіальну підшкірну вену руки. Крім того, успішність емболектомії була низькою при застосуванні синтетичного протеза.
Background. For hemodialysis, an autogenous radiocephalic or brachiocephalic fistula is the preferred types of vascular access, while basilic vein transposition (BVT) fistula followed by prosthetic grafting is suggested if unsuitable veins are present. The purpose was to compare the outcome of BVT versus synthetic vascular graft used for dialysis in a single centre. Materials and methods. This study includes total of 148 patients that subdivided into two groups: group one (n = 127; 69 male and 58 female patients, mean age 49 years) operated with BVT and group two (n = 21; 15 male and 6 female individuals, mean age 58 years) operated with synthetic vascular graft. Results. Seven patients with hematoma were treated with exploration within 7 days of operation (p = 0.001). Venous hypertension was present in 3 patients of group one and no patient in group two (p = 0.001). In group one, the complication rate was 13.38 %, while in group two, it was 28.57 % with statistically significant difference (p = 0.001). In group one, primary patency rate is 96.85 versus 90.47 % in group two (p = 0.07). The assisted primary in group one was 75 % versus no patient assisted in group two (p = 0.001). Conclusions. This study concludes that use of synthetic graft for dialysis is associated with more complications regarding thrombosis rate, ischemic steal syndrome and infection rate compared to using the basilic vein. In addition to that, the successful rate of embolectomy was low with synthetic graft use.
гемодіаліз; медіальна підшкірна вена руки; синтетичний протез; хронічні захворювання нирок
hemodialysis; basilic vein; synthetic graft; chronic kidney disease
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Segura-Orti E, Koufaki P, Kouidi E. Bridging the gap from research to practice for enhanced health-related quality of life in people with chronic kidney disease. Clin Kidney J. 2021;14(Suppl 2):ii34-ii42. doi: 10.1093/ckj/sfaa268.
- Kakkos SK, Lampropoulos GC, Nikolakopoulos KM, Tsolakis IA, Papadoulas SI, et al. A systematic review and meta-analysis of randomized trials comparing two-stage with one-stage brachio-basilic vein fistulas. Vasc Specialist Int. 2018;34(3):51-60. doi: 10.5758/vsi.2018.34.3.51.
- Noori N, Sharma Parpia A, Wald R, Goldstein MB. Validation of the SMH equations for the estimation of the total body water volume in hemodialysis patients. Can J Kidney Health Dis. 2022;9:20543581221137180. doi: 10.1177/20543581221137180.
- Porazko T, Piersiak A, Klinger M. The efficacy of single suture for exit site wound closure and stabilization of hemodialysis central tunneled catheter. SAGE Open Med. 2021;9:20503121211019889. doi: 10.1177/20503121211019889.
- Almhanni G, Sen I, Vang S, Marczak S, Herzog K, et al. Midterm outcomes of endoscopic-assisted brachial-basilic arteriovenous fistula creation. J Vasc Surg Cases Innov Tech. 2023;10(2):101382. doi: 10.1016/j.jvscit.2023.101382.
- Lu Y, Xiao J, Liu C, Wang Y. Comparison of wound complications between one-stage and two-stage brachiobasilic arteriovenous fistula: A meta-analysis. Int Wound J. 2023;20(9):3786-3793. doi: 10.1111/iwj.14278.
- Li H, Jen S, Ramayya T, Bowers HG, Rotem E. Unanticipa–ted late maturation of an arteriovenous fistula after creation of separate graft access. Quant Imaging Med Surg. 2018;8(4):444-446.
- Al Shakarchi J, Houston G, Inston N. Early cannulation grafts for haemodialysis: a systematic review. J Vasc Access. 2015;16(6):493-497.
- Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev. 2015;7:CD002786.
- Migliori M, Cantaluppi V, Scatena A, Panichi V. Antiplatelet agents in hemodialysis. J Nephrol. 2017;30(3):373-383. doi: 10.1007/s40620-016-0367-5.
- Iglesias R, Lodi M, Rubiella C, Teresa Parisotto M, Ibeas J. Ultrasound guided cannulation of dialysis access. J Vasc Access. 2021;22(1_suppl):106-112. doi: 10.1177/11297298211047328.
- Kaller R, Russu E, Arbănași EM, Mureșan AV, Jakab M, et al. Intimal CD31-positive relative surfaces are associated with systemic inflammatory markers and maturation of arteriovenous fistula in dialysis patients. J Clin Med. 2023;12(13):4419. doi: 10.3390/jcm12134419.
- Deguchi J, Sato O. Transposed brachial-basilic arteriovenous fistula for vascular access in Japan. Ann Vasc Dis. 2018;11(2):181-190. doi: 10.3400/avd.ra.18-00009.
- Patel RJ, Willie-Permor D, Zarrintan S, Elsayed N, Al-Nouri O, Malas MB. Two-stage offers no advantages over single-stage arteriovenous creation: An analysis of multicenter national data. Ann Vasc Surg. 2023;96:308-315. doi: 10.1016/j.avsg.2023.03.020.
- Kakkos SK, Tsolakis IA, Papadoulas SI, Lampropoulos GC, Papachristou EE, et al. Randomized controlled trial comparing primary and staged basilic vein transposition. Front Surg. 2015;2:14. doi: 10.3389/fsurg.2015.00014.
- Sadasivan K, Kunjuraman U, Murali B, Yadev I, Kochunarayanan A. Factors affecting the patency of radiocephalic arteriovenous fistulas based on clinico-radiological parameters. Cureus. 2021;13(3):e13678. doi: 10.7759/cureus.13678.
- Sadeghi A, Setayesh Mehr M, Esfandiari E, Mohammadi S, Baharmian H. Variation of the cephalic and basilic veins: A case report. J Cardiovasc Thorac Res. 2017;9(4):232-234. doi: 10.15171/jcvtr.2017.40.
- Van Dellen D, Junejo M, Khambalia H, Campbell B. Transposition of brachiobasilic arteriovenous fistulae: improving the cosmetic effect without compromising patency. Ann R Coll Surg Engl. 2016;98(1):24-28. doi: 10.1308/003588414X14055925061757.
- Laranjinha I, Matias P, Azevedo A, Navarro D, Ferreira C, et al. Are high flow arteriovenous accesses associated with worse haemodialysis? J Bras Nefrol. 2018;40(2):136-142. doi: 10.1590/2175-8239-JBN-3875.
- Moosa MA, Shaikh FA, Ali M, Salam A, Sophie Z, Siddiqui N. Comparison of upper limb translocated femoral vein and prosthetic arteriovenous bridge grafts. Cureus. 2019;11(11):e6219. doi: 10.7759/cureus.6219.
- Xiao Y, Vazquez-Padron RI, Martinez L, Singer HA, Woltmann D, Salman LH. Role of platelet factor 4 in arteriovenous fistula maturation failure: What do we know so far? J Vasc Access. 2024;25(2):390-406. doi: 10.1177/11297298221085458.
- Jairath A, Singh A, Sabnis R, Ganpule A, Desai M. Minimally invasive basilic vein transposition in the arm or forearm for auto–genous haemodialysis access: A less morbid alternative to the conventional technique. Arab J Urol. 2017;15(2):170-176. doi: 10.1016/j.aju.2017.01.004.
- Jeong H, Bae M, Chung SW, Lee CW, Huh U, Kim MS. Videoscopic surgery for arteriovenous hemodialysis access. Korean J Thorac Cardiovasc Surg. 2020;53(1):28-33. doi: 10.5090/kjtcs.2020.53.1.28.
- Kahraman N, Demir D. Outcomes of arteriovenous fistula reconstruction in vascular access dysfunction. Am J Transl Res. 2019;11(2):1058-1065.
- Saroukhani A, Rafiee Zadeh A, Ahmadi SM. Incidence of steal syndrome following arteriovenous fistula and arteriovenous graft. Int J Burns Trauma. 2022;12(3):121-126.
- Lookstein RA, Haruguchi H, Ouriel K, Weinberg I, Lei L, Cihlar S, Holden A; IN.PACT AV Access Investigators. Drug-coated balloons for dysfunctional dialysis arteriovenous fistulas. N Engl J Med. 2020;383:733-742.
- Karaca OG, Basal AN, Ecevit AN, Kalender M, Darcin OT, Sungur MA. Radiobasilic versus brachiobasilic transposition on the upper arm to avoid steal syndrome. Med Sci Monit. 2015;21:4090-4095.
- Sepas HN, Negahi A, Mousavie SH, Vosough F, Farazmand B. Patency and outcomes of tunneled hemodialysis catheter via femoral versus jugular vein access. J Adv Pharm Technol Res. 2019;10(2):81-84. doi: 10.4103/japtr.JAPTR_383_18.
- Solanki PB. Autologous vein graft in living donor kidney transplant (case report). Kidneys. 2024;13(2):172-174. doi: 10.22141/2307-1257.13.2.2024.457.
- Ivanova M. The role of levocarnitine in the systemic the–rapy of patients of different profiles on chronic hemodialysis. Kidneys. 2022;(1.07):81-84. doi: 10.22141/2307-1257.0.1.07.2014.76553.