
Журнал «Здоровье ребенка» 4 (64) 2015
Вернуться к номеру
Create mathematics model food allergy in the childrens illness bronchial asthma
Авторы: Levitsky V.M., Yurchyshena E.V., Yurchyshen O.M., Mysko L.V., Mysko U.L. - Мunicipal Children Hospital , Khmelnytskyi, Ukraine
Рубрики: Педиатрия/Неонатология
Разделы: Справочник специалиста
Версия для печати
Introduction. In the occurrence and persistence of asthma (BA) in children occupy a significant place factors that are inducing effect (exogenous specific chyynyky - allergens) that vary during disease in one patient, and can be combined. Against the background of genetic susceptibility to asthma trigger these exogenous factors cause inflammation in the bronchi and / or acute bronchoconstriction, and for infants leading role among these "launching" factors play food allergens [1]. In early childhood food allergy (HA) has considerable polymorphism, which is not only of - "targets", but the clinical severity of the pathological process from anaphylaxis to disguised forms [5].
Every year prevalence of allergic diseases among children is increasing, and the terms of allergic reactions and diseases steadily approaching date of birth. "Pomolodshannya" allergic disease has led to a shift in the peak incidence of early age at which HA occupies a leading place in the structure of allergic disease. HA is the first manifestation of a genetic predisposition to the development of atopy and trigger factor in the development of respiratory, skin, gastrointestinal manifestations [6]. The clinical picture of AD in infants and preschool children is characterized by variability in the course of severe acute subclinical forms to [4] or disguised [8]. In addition, the emphasis changed in the treatment of allergic diseases, including asthma who zsunulysya towards preventive measures mizhnapadnomu period and are in the recovery environment sick child, seizure cause - significant allergens [9]. In view of this, the identification of AD patients with asthma to eliminate from their diet cause - significant allergen probably can not only facilitate trofalerhiyi course, but also reduce the severity and number of attacks of asthma.
Rezudtaty research and discussion. BA is one of the most common childhood diseases [5] and the most common allergic respiratory diseases in children [1], which is inherent in "pomolodshannya" in recent years [2] with the formation and consolidation of bronchial hyperreactivity at an early age, particularly in the first year life. Investigation of the role of atopic constitution in the development of asthma in children in recent years have distinguished the opening of atopy gene localized on chromosome 11, and the verification of some paraclinical markers, including certain HLA - antigens [3], which is associated with the development of atopic asthma later in children . The development of asthma in children is closely linked to the complex genetic and environmental factors. In etiological (sensitizing) allergens action on the child in the development of asthma are important precipitating factors that cause acute illness, and at present these factors are not limited exclusively aeroalerhenamy [7]. Thus, removal of the diet of the children in some obligate food allergens leads to reduction in the incidence of bronchial obstruction in patients with atopic constitution.
However, high levels of sensitization to trofalerheniv, according to other authors [1], only 7.2% of patients pubertal age was important trigger factor in the development of bronchial obstruction, and in preschoolers causal significance in the development of asthma becomes polyvalent allergy [2]. BA common among children, is an early "start" bronchial obstruction syndrome, so it is important to improve methods of detection disguised HA in patients with asthma to improve the treatment of these patients by eliminating exposure to cause - significant in the development of asthma food allergens.
Therefore, to develop diagnostic criteria for detection of concealed AD in children with asthma, we conducted a comprehensive survey of 100 young child and preschool children suffered from asthma. Formed two clinical comparison groups: the first (I) basic group consisted of 50 children who have asthma ran across on the background of HA, the second (II) comparison group consisted of 50 children with asthma without HA. Groups were formed on the basis of random selection. When creating clinical groups hrupoformuyuchoyu feature was the presence in patients with complex diagnostic signs on HA - clinical manifestations of hypersensitivity to food history combined with high positive intradermal tests with food allergens, such as rizkopozytyvni evaluated and the presence of serum specific to trofalerheniv immunoglobulin E (IgE).
Thus, the main clinical characteristics of children were zistavymi comparison groups.
To create a mathematical model of AD diagnosis in infants and preschool children suffering from asthma, conducted multivariate dispersion and regression analyzes of complex clinical - paraclinical examination of patients included in the clinical comparison group.
Research the main components of the structure HA diagnosis using multivariate analysis of key indicators of clinical observation of children, the clinical history and paraclinical features, helped to create the factor structure of clinical -paraklinichnoho model AD in children with asthma.
Thus, our multivariate analysis revealed the factor structure of the diagnosis of AD in children with asthma using basic components, which covered the results of clinical - paraclinical examination of patients and were pronounced, statistically significant correlations with this nosological forms.
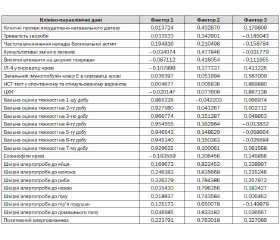
The method of analysis of variance installed cumulative significance of selected factors in identifying AD patients early and preschool children suffering from asthma. Thus, the first factor is the cumulative index values (variance) of 32.3%, which is about 1/3 includes components necessary for the mathematical description of HA. The second factor (F2) adds to the description of this diagnosis is 19%, so the first two factors are cumulative significance of 51.3%. The cumulative value of F3 defines this diagnosis by using an existing 60.0% of the components that can be used in the diagnostic process. Given that criteria Neyzera for all studied factors exceeded 1.0, indicating their importance and the significance, imagined advisable to include them in the analysis of principal components regression in AD patients studied to predict this nosology based on the mathematical model of children patients with asthma.
The method of multiple regression established clinical - paraclinical image HA in children with asthma using specified by us in the previous step analysis of the main components of multivariate analysis of this disease, which can be represented by the following mathematical formula.
The coefficient of multiple correlation developed mathematical models of AD in children surveyed was 0.93, which accurately reflects not only the mathematical model, but also allows to predict this pathology in patients early and preschool children suffering from asthma. Thus, if a child of the constellations selected indicators can be a statistical certainty and precision (coefficient of determination = 0.86) to predict the presence of a child suffering from asthma food allergies, which can be represented as a mathematical formula.
The study features of bronchial obstruction syndrome in children surveyed who had symptoms of AD on admission to hospital and during treatment within the first 4 - days revealed no plausible differences depending on the characteristics of the history and clinical - paraclinical examination results. This, in our opinion, indicates that the course of bronchial obstruction in children with asthma have their patterns of development that does not affect the course of AD.
Thus, based on our multivariate analysis of clinical diagnosis -paraklinichnyh component structure in AD patients with asthma infants and preschool children, marked the most significant of them that can be used in the mathematical model, which not only describe this nosology, but also to predict its availability.
Conclusions:
1. Investigation of the main components of the structure of the diagnosis of food allergy using multivariate analysis of key indicators of clinical observation of children helped to create the factorial structure of clinical - paraclinical model of AD in children with asthma.
2. A multivariate analysis revealed the factor structure of the diagnosis of food allergy in children with asthma using basic components, which covered the results of clinical - paraclinical examination of patients and were pronounced, statistically significant correlations with this nosological forms.
3. The method of analysis of variance installed cumulative significance of selected factors to identify food allergies in patients early and preschool children with bronchial asthma.
4. The method of multiple regression established clinical - paraclinical image of food allergy in children with asthma identified using principal components analysis of multivariate this disease.