
Журнал "Гастроэнтерология" Том 56, №4, 2022
Вернуться к номеру
Клініко-ендоскопічні й біохімічні паралелі хронічних запальних захворювань кишечника з позитивними маркерами запалення
Авторы: Степанов Ю.М., Тарасова Т.С., Стойкевич М.В., Сімонова О.В., Татарчук О.М.
ДУ «Інститут гастроентерології НАМН України», м. Дніпро, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
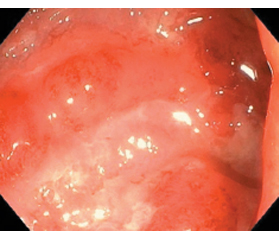
Актуальність. Поширеність запальних захворювань кишечника (ЗЗК) на сьогодні зростає в усьому світі та являє собою серйозну проблему, що обумовлює цікавість до її вивчення, особливо до розробки менш інвазивних діагностичних заходів. У дослідженнях останніх років, присвячених діагностиці ЗЗК, зустрічаються дані, що вказують на можливість використання IgG4 як діагностичного біомаркера. Мета: дослідити особливості ендоскопічних проявів і активності ЗЗК залежно від тяжкості перебігу захворювання, рівнів фекального кальпротектину (ФК) та IgG4. Матеріали та методи. Обстежено 100 хворих на ЗЗК, у тому числі 75 пацієнтів з виразковим колітом (ВК) і 25 — з хворобою Крона (ХК). Пацієнти були розподілені на групи залежно від нозології і тяжкості перебігу. Усім пацієнтам виконувалось ендоскопічне дослідження з метою верифікації діагнозу, визначався рівень IgG, IgG4 у сироватці крові, співвідношення IgG4/IgG і значення фекального кальпротектину. Результати. Встановлено суттєве зростання ступеня ендоскопічної активності разом з посиленням тяжкості перебігу виразкового коліту й хвороби Крона. Встановлено, що рівень ФК збільшувався зі зростанням ступеня тяжкості ВК і ХК. У хворих на ВК і ХК встановлено вірогідне зниження рівня IgG (р < 0,05). Концентрація IgG4 у групі хворих на ВК була вище у 2,3 раза (р < 0,05) і 2,5 раза (р < 0,05) порівняно із його рівнем у групі контролю і хворих на ХК відповідно. Встановлено кореляційний зв’язок рівня IgG4 з індексом Беста, ступенем тяжкості, локалізацією запального процесу в товстій кишці, співвідношенням IgG4/IgG. Встановлено зв’язок співвідношення IgG4/IgG з ендоскопічним індексом активності ЗЗК і сироватковим IgG4. Висновки. Ступінь ендоскопічної активності ЗЗК зростав разом з тяжкістю перебігу захворювання. Встановлено позитивний кореляційний зв’язок між рівнем ФК і ступенем тяжкості ЗЗК і обернений кореляційний зв’язок з рівнем IgG. Рівень IgG4 залежав від ендоскопічної активності ЗЗК, що підтверджено кореляційним зв’язком. Виявлено підвищення концентрації IgG4 у сироватці крові у хворих на ВК у 2 рази (р < 0,05) і 2,5 раза (р < 0,05) порівняно з його рівнем у групі контролю і хворих на ХК відповідно. Отримані дані можуть бути використані для диференціальної діагностики між ВК і ХК.
Background. The prevalence of inflammatory bowel disease (IBD) is currently increasing worldwide and represents a serious problem that causes interest in the study and, especially, in the development of less invasive diagnostic measures. In the studies of years on the diagnosis of IBD, there are data indicating the possibility of using IgG4 as a diagnostic biomarker. Purpose: to investigate the peculiarities of endoscopic manifestations and activity of IBD depending on the disease severity, the levels of fecal calprotectin (FC) and IgG4. Materials and methods. One hundred patients with IBD were examined, including 75 people with ulcerative colitis (UC) and 25 with Crohn’s disease (CD). Patients were divided into groups depending on the nosology and severity of the course. All of them underwent an endoscopic examination to verify the diagnosis; the level of IgG, IgG4 in blood serum, the IgG4/IgG ratio, and the content of FC were determined. Results. A significant increase in the degree of endoscopic activity was detected along with an increase in the severity of ulcerative colitis and Crohn’s disease. It was found that the level of FC increased with increasing severity of UC and CD. In patients with UC and CD, a probable decrease in the level of IgG was revealed (p < 0.05). The concentration of IgG4 in the group of patients with UC was 2.3 (p < 0.05) and 2.5 times (p < 0.05) higher compared to the control group and patients with CD, respectively. A correlation was found between the level of IgG4 and the index of Best, the degree of severity, the localization of the inflammatory process in the colon, and the ratio of IgG4/IgG. The relationship of the IgG4/IgG ratio with the endoscopic index of IBD activity and serum IgG4 was revealed. Conclusions. The degree of endoscopic activity of IBD increased along with the severity of the disease. A positive correlation was found between the FC level and the severity of IBD and an inverse correlation — with IgG level. The level of IgG4 depended on the endoscopic activity of IBD, which was confirmed by a correlation. A 2-fold (p < 0.05) and 2.5-fold (p < 0.05) increase was found in the concentration of IgG4 in the blood serum of patients with UC compared to the control group and patients with CD, respectively. The obtained data can be used for differential diagnosis of UC and CD.
запальні захворювання кишечника; фекальний кальпротектин; IgG; IgG4; ендоскопічна активність
inflammatory bowel diseases; fecal calprotectin; IgG; IgG4; endoscopic activity
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ye Y., Pang Z., Chen W., Ju S., Zhou C. The epidemiology and risk factors of inflammatory bowel disease. Int J Clin Exp Med. 2015. Vol. 8. Р. 22529-22542.
- Sartor R.B. Current concepts of the etiology and pathogenesis of ulcerative colitis and Crohn’s disease. Gastroenterol Clin N Am. 1995. Vol. 24. Р. 475-507.
- The innate and adaptive immune system as targets for biologic therapies in inflammatory bowel disease / Holleran G. et al. Int J Mol Sci. 2017. Vol. 18(10). Р. 2020. Published 2017 Sep 21. DOI: 10.3390/ijms18102020.
- Lichtenstein G.R., McGovern D.P.B. Using markers in IBD to predict disease and treatment outcomes: rationale and a review of current status. Am J Gastroenterol Suppl. 2016. Vol. 3. Р. 17-26.
- Panes J., Jairath V., Levesque B.G. Advances in use of endoscopy, radiology, and biomarkers to monitor inflammatory bowel diseases. Gastroenterology. 2017. Vol. 152. Р. 362-373.
- Kamisawa T., Zen Y., Pillai S., Stone J.H. IgG4-related di–sease. Lancet. 2015. Vol. 385. Р. 1460-1471. DOI: 10.1016/S0140-6736(14)60720-0.
- IgG4 characteristics and functions in cancer immunity / Crescioli S. et al. Curr Allergy Asthma Rep. 2016. Vol. 16. Р. 7. DOI: 10.1007/s11882-015-0580-7.
- Stone J.H., Zen Y., Deshpande V. IgG4-related disease. N Engl J Med. 2012. Vol. 366. Р. 539-551. DOI: 10.1056/NEJMra1104650.
- Shen B., Bennett A.E., Navaneethan U. IgG4-associated pouchitis. Inflamm Bowel Dis. 2011. Vol. 17. Р. 1247-1248. DOI: 10.1002/ibd.21441.
- Elevated serum IgG4 is associated with chronic antibiotic-refractory pouchitis / Navaneethan U. et al. J Gastrointest Surg. 2011. Vol. 15. Р. 1556-1561. DOI: 10.1007/s11605-011-1587-6.
- Immunoglobulin G4 Immunostaining of Gastric, Duodenal, or Colonic Biopsies Is Not Helpful for the Diagnosis of Autoimmune Pancreatitis / Rebours V. et al. Clin Gastroenterol Hepatol. 2012. Vol. 10. Р. 91-94. DOI: 10.1016/j.cgh.2011.09.008.
- Mucosal IgG4 cell infiltration in ulcerative colitis is linked to disease activity and primary sclerosing cholangitis / Raina A. et al. Inflamm Bowel Dis. 2013. Vol. 19. Р. 1232-1237. DOI: 10.1097/MIB.0b013e318281344d.
- High level of IgG4 as a biomarker for a new subset of inflammatory bowel disease / Wang Z. et al. Sci Rep. 2018. Vol. 8(1). Р. 10018. Published 2018 Jul 3. DOI: 10.1038/s41598-018-28397-8.
- Histopathological diagnostic value of the IgG4(+)/IgG(+) ratio of plasmacytic infiltration for IgG4-related diseases a PRISMA-compliant systematic review and meta-analysis / Deng C. et al. Medicine. 2015. Vol. 94. e579. DOI: 10.1097/MD.0000000000000579.
- The combined measurement of total serum IgG and IgG4 may increase diagnostic sensitivity for autoimmune pancreatitis without sacrificing specificity, compared with IgG4 alone / Song T.J. et al. Am J Gastroenterol. 2010. Vol. 105. Р. 1655-1660. DOI: 10.1038/ajg.2009.689.
- Lehman J.S., Smyrk T.C., Pittelkow M.R. Increased immunoglobulin (Ig) G4-positive plasma cell density and IgG4/IgG ratio are not specific for IgG4-related disease in the skin. Am J Clin Pathol. 2014. Vol. 141. Р. 234-238. DOI: 10.1309/AJCPTMWTCN04GSJH.
- Псарьова І.В. Зв’язок біомаркерів запалення в товстій кишці з індексами активності неспецифічного виразкового коліту. Гастроентерологія. 2020. Т. 54. № 1. С. 38-43. doi: 10.22141/2308-2097.54.1.2020.199140.
- Степанов Ю.М., Скирда І.Ю., Петішко О.П. Хронічні запальні захворювання кишечника: особливості епідеміології в Україні. Гастроентерологія. 2017. Т. 51. № 2. С. 11-19.
- Jukic A., Bakiri L., Wagner E.F., Tilg H., Adolph T.E. Calprotectin: from biomarker to biological function. Gut. 2021 Oct. 70(10). 1978-1988. doi:10.1136/gutjnl-2021-324855.
- Минимальная стандартная терминология в эндоскопии пищеварительной системы / Е.Д. Федоров и др. Москва: Интел-Синтез, 2001. 80 с.