
Журнал «Медицина неотложных состояний» Том 19, №2, 2023
Вернуться к номеру
Аналіз серії клінічних випадків із застосуванням ад’ювантів до загальної анестезії при плановому кесаревому розтині
Авторы: Падалко А.А. (1), Дзюба Д.О. (2, 3), Галушко О.А. (3)
(1) — КНП КОР «Київський обласний перинатальний центр», м. Київ, Україна
(2) — КНП КОР «Київська обласна клінічна лікарня», м. Київ, Україна
(3) — Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
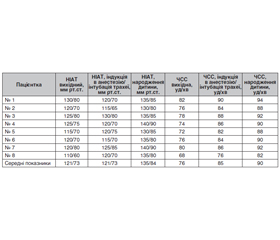
Актуальність. Кесарів розтин залишається одним із найчастіших оперативних втручань у всьому світі. Основними недоліками загальної анестезії при кесаревому розтині є: високий рівень ймовірності збереження свідомості під час операції і виражена гемодинамічна реакція на операційну травму у пацієнтки. Найнебезпечнішим періодом оперативного втручання щодо виникнення цих ускладнень є період до народження дитини. У статті проведено аналіз власних клінічних випадків загальної анестезії при кесаревому розтині з додаванням ад’ювантів та порівняння анестезіологічного менеджменту зі світовими практиками. У всіх випадках власної клінічної практики проводилась тотальна внутрішньовенна анестезія зі штучною вентиляцією легень. Як ад’юванти було застосовано внутрішньовенні форми медичних препаратів: парацетамол (1000 мг) і клонідин (100 мкг) за 30 хвилин до планового оперативного втручання. Проводилась оцінка новонародженого за шкалою Апгар і аналіз газів пуповинної венозної крові. Передопераційний, інтраопераційний та післяопераційний менеджмент пацієнтів базувався на рекомендаціях з раннього відновлення після операції кесаревого розтину та рекомендаціях робочої групи PROSPECT. Результати аналізу власних клінічних випадків: виявилено наявність гемодинамічної реакції організму пацієнта на операційну травму (у періоді до народження дитини), що не перевищує безпечні рівні; відсутність анестезіологічних ускладнень та випадків збереження свідомості пацієнта під час оперативного втручання; відсутність негативного впливу ад’ювантів на новонароджених; достатній рівень глибини анестезії та зменшення доз застосованих інтраопераційно наркотичних анальгетиків і внутрішньовенних анестетиків («на потребу пацієнта»). Висновки. Аналіз клінічних випадків аргументує необхідність застосування «безпечних ад’ювантів» (ацетамінофен, клонідин) до загальної анестезії при плановому кесаревому розтині та необхідність подальших досліджень.
Background. Caesarean section remains one of the most common surgical interventions in the world. The main disadvantages of the general anesthesia in caesarean section are a high risk of awareness during the operation and a pronounced hemodynamic reaction to the surgical trauma in a patient. The most dangerous period of intervention in terms of these complications is the period before the birth of a child. This article analyzes our own clinical cases of the general anesthesia during elective caesarean section with the addition of adjuvants and compares anesthetic management with world practices. In all cases from our own clinical practice, total intravenous anesthesia with artificial lung ventilation was performed. Intravenous forms of medical drugs were used as adjuvants: paracetamol (1000 mg) and clonidine (100 μg), 30 minutes before the elective surgical intervention. The newborns were examined with the Apgar scale and umbilical venous blood gas analysis was carried out. Preoperative, intraoperative, and postoperative management of patients was based on recommendations of the Enhanced Recovery After Caesarean Section and guidelines of the PROSPECT working group. Results. The analysis of our own clinical cases revealed the presence of a hemodynamic reaction of the patient’s body to the operative injury (in the period before the birth of a child), which does not exceed safe levels; absence of anesthetic complications and cases of accidental awareness during surgery; absence of a negative influence of adjuvants on newborns; sufficient depth of anesthesia and reduction of the intraoperative doses of opioids and intravenous anesthetics (“on patient’s request”). Conclusions. The analysis of clinical cases argues for the need to use “safe adjuvants” (acetaminophen, clonidine) to general anesthesia during elective caesarean section and the necessity for further research.
загальна анестезія; тотальна внутрішньовенна анестезія; штучна вентиляція легень; кесарів розтин; клонідин; ацетамінофен
general anesthesia; total intravenous anesthesia; artificial lung ventilation; caesarean section; clonidine; acetaminophen
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ala-Kokko T.I., Pienimaki P., Lampela E. et al. Transfer of clonidine and dexmedetomidine across the isolated perfused human placenta. Acta Anaesthesiol. Scand. 1997. 41. 313-319.
- American Society of Anesthesiologists Task Force on Intraoperative Practice advisory for intraoperative awareness and brain function monitoring: a report by the Аmerican society of anesthesiologists task force on intraoperative awareness. Anesthesiology. 2006. 104 (4). 847-64. doi: 10.1097/00000542-200604000-00031 [PubMed: 16571982].
- Betrán A.P., Ye J., Moller A.B. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLOS One. 2016. 11. 2. e0148343.
- Bilgen S., Koner O., Ture H. Effect of three different doses of ketamine prior to general anaesthesia on postoperative pain following Caesarean delivery: a prospective randomized study. Minerva Anestesiol. 2012. 78. 4. 442-449.
- Bollag L., Lim G., Pervez S., Habib A. et al. Society for Obstetric Anesthesia and Perinatology: Consensus Statement and Recommendations for Enhanced Recovery After Cesarean. Anesth. Analg. 2021 May 1. 132 (5). 1362-1377.
- Brown J.P.R. Recent developments in anaesthesia for caesarean section in the UK. Update Anaesth. 2008. 23. 3-7.
- Buchanan M.L., Easterling T.R., Carr D.B. et al. Clonidine pharmacokinetics in pregnancy. Drug Metab. Dispos. 2009. 37 (4). 702-705.
- Chin K.J., Yeo S.W. A BIS-guided study of sevoflurane requirements for adequate depth of anaesthesia in Caesarean section. Anaesthesia. 2004. 59. 1064-1068.
- Datta S., Kodali B.S., Segal S. Obstetric Anesthesia Handbook. 5th ed. New York: Springer-Verlag, 2010. 488 p.
- Deschenes G., Gosselin J., Couture M. Interobserver reliabi–lity of the Amiel-Tison neurological assessment at term. Pediatr. Neurol. 2004. 30. 3. 190-194.
- Devroea S., Marc Van de Veldea, Rex S. General anesthesia for caesarean section. Curr. Opin. Anesthesiol. 2015. 28. 240-246. DOI: 10.1097/ACO.0000000000000185.
- Dünges B., Heid F., Dauster M. et al. Revisited: Haemodynamic instability and endocrine response during endotracheal tube-placement. A prospective, randomized trial using topical lidocaine and a lightwand. Open Anesthesiol. J. 2008. 2. 30-9. doi: 10.2174/1874321800802010030.19.
- Ebneshahidi A., Mohseni M. Premedication with oral clonidine decreases intraoperative bleeding and provides hemodynamic stability in cesarean surgery section. Anesth. Pain. 2011. 1. 30-3.
- FDA News Release. FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products. Accessed August 1, 2019 at https://www.fda.gov/drugs/labeling/pregnancy-and-lactation-labeling-drugs-final-rule.
- Fehr S.B., Zalunardo M.P., Seifert B. et al. Clonidine decreases propofol requirements during anaesthesia: effect on bispectral index. Br. J. Anaesth. 2001. 86 (5). 627-32. doi: 10.1093/bja/86.5.627 [PubMed: 11575336].
- Flaishon R., Windsor A., Sigl J. et al. Recovery of consciousness after thiopental or propofol. Bispectral index and isolated forearm technique. Anesthesiology. 1997. 86. 613-9.
- Glass P.S., Bloom M., Kearse L. et al. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane and alfentanil in healthy volunteers. Anesthesiology. 1997. 86. 836-47.
- Guasch E., Montenegro P., Ochoa C. General anaesthesia and obstetric bleeding in caesarean section. One year’s experience in a university hospital. Rev. Esp. Anestesiol. Reanim. 2012. 59. 8. 415-422.
- Hagberg C., Georgi R., Krier C. Complications of managing the airway. Best Pract. Res. Clin. Anaesthesiol. 2005. 19. 641-59.
- Hall J.E., Uhrich T.D., Ebert T.J. Sedative, analgesic and cognitive effects of clonidine infusions in humans. Br. J. Anaesth. 2001. 86 (1). 5-11. doi: 10.1093/bja/86.1.5 [PubMed: 11575409].
- Hamilton B.E., Martin J.A., Osterman M.J. Birth: Preliminary data for 2014. National Vital Statistics Reports. 2014. 64. 6. 1-19.
- Hassani V., Movassaghi G., Goodarzi V. et al. Comparison of fentanyl and fentanyl plus lidocaine on attenuation of hemodynamic responses to tracheal intubation in controlled hypertensive patients undergoing general anesthesia. Anesth. Pain Med. 2013. 2. 115-8.
- Hawkins J.L., Chang J., Palmer S.K. Anesthesia-Related Maternal Mortality in the United States: 1979–2002. Obstet. Gynecol. 2011. 117. 1. 69-74.
- Hawkins J.L., Gibbs C.P., Orleans M. Obstetric Anesthesia Work Force Survey, 1981 versus 1992. Anesthesiology. 1997. 87. 1. 135-143.
- Heesen M., Klohr S., Hofmann T., Van de Velde M. et al. Maternal and foetal effects of remifentanil for general anaesthesia in parturients undergoing caesarean section: a systematic review and meta-analysis. Acta. Anaesthesiol. Scand. 2013. 57. 29-36.
- Horvath J.S., Phippard A., Korda A. et al. Clonidine hydrochloride — a safe and effective antihypertensive agent in pregnancy. Obstet. Gynecol. 1985. 66 (5). 634-638.
- Huang C.J., Fan Y.C., Tsai P.S. Differential impacts of modes of anesthesia on the risk of stroke among preeclamptic women who undergo Caesarean delivery: a population-based study. Br. J. Anaesth. 2010. 105. 818-26. 30.
- Kearse L.A. Jr., Rosow C., Zaslavsky A. et al. Bispectral analysis of the electroencephalogram predicts conscious processing of information during propofol sedation and hypnosis. Anesthesiology. 1998. 88. 25-34.
- Khan F.A., Ullah H. Pharmacological agents for preventing morbidity associated with the hemodynamic response to tracheal intubation. Cochrane Database Syst. Rev. 2013. 7. CD004087. doi: 10. 1002/14651858. CD004087. pub2.
- Khan Z.H. Preeclampsia-eclampsia: an insight into the dilemma of treatment by the anesthesiologist. Acta. Med. Iran. 2011. 49. 564-74.
- Kinsella S.M. A prospective audit of regional anaesthesia fai–lure in 5080 caesarean sections. Obstet. Gynecol. Surv. 2008. 63. 12. 752-762.
- Kutlesic M., Kutlesic R., Koracevic G. Significance, etiology and prevention of venous thromboembolism in pregnancy and puerperium. Vojnosanit. Pregl. 2014. 71. 580-7. 27.
- Landau R., Bollag L., Ortner C. Chronic pain after childbirth. International Journal of Obstetric Anesthesia. 2013. 22. 2. 133-145.
- Landoni G., Rodseth R.N., Santini F. [et al.]. Randomized evidence for reduction of perioperative mortality. J. Cardiothorac. Vasc. Anesth. 2012. 26. 5. 764-72.
- Lee D.H., Kwon I.C. Magnesium sulphate has beneficial effects as an adjuvant during general anaesthesia for Caesarean section. Br. J. Anaesth. 2009. 103. 861-6.
- Lin S.Y., Hu C.J., Lin H.C. Increased risk of stroke in patients who undergo cesarean section delivery: a nationwide population based study. Am. J. Obstet. Gynecol. 2008. 98. 391. e1-7. 28.
- Littleford J. Effects on the fetus and newborn of maternal analgesia and anesthesia: a review. Can. J. Anesth. 2004. 51. 586-609.
- Liu J., Singh H., White P.F. Electroencephalogram bispectral analysis predicts the depth of midazolam-induced sedation. Anesthesiology. 1996. 84. 64-9.
- Lumbiganon P., Laopaiboon M., Gülmezoglu A.M. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007–08. The Lancet. 2010. 375. 9713. 490-499.
- Lymperopoulos A. Physiology and pharmacology of the cardiovascular adrenergic system. Front Physiol. 2013. 4. 240.
- Ma D., Rajakumaraswamy N., Maze M. Alpha-2-Adrenoceptor agonists: shedding light on neuroprotection? Br. Med. Bull. 2005. 71. 77-92.
- Maronge L., Bogod D. Complications in obstetric anaesthesia. Anaesthesia. 2018. 73. Suppl. 1. 61-66.
- Mehdi Rajabi, Mohammad-Reza Razavizade et al. Magnesium Sulfate and Clonidine; Effects on Hemodynamic Factors and Depth of General Anesthesia in Cesarean Section. Anesth. Pain. Med. 2020 October. 10 (5). e100563. doi: 10.5812/aapm.100563.
- Menigaux C., Guignard B., Adam F. et al. Esmolol prevents movement and attenuates the BIS response to orotracheal intubation. Br. J. Anaesth. 2002. 89. 857-62.
- Mi J., Liu F. Rate of caesarean section is alarming in China. The Lancet. 2014. 383. 9927. 1463-1464.
- Millar J., Williams G.V. Effect of iontophoresis of noradrenaline and stimulation of the periaqueductal gray on single-unit activity in the rat superficial dorsal horn. J. Comp. Neurol. 1989. 287. 1. 119-33.
- Miller R.D. Monitoring the depth of anesthesia. Millers Anesth. 2010. 39. 1241.
- Montazeri K., Kashefi P., Honarmand A. et al. Attenuation of the pressor response to direct laryngoscopy and tracheal intubation: oral clonidine vs. oral gabapentin premedication. J. Res. Med. Sci. 2011. 16. 377-86. 21.
- Morris J., Acheson M., Reeves M. et al. Effect of clonidine premedication on propofol requirements during lower extremity vascular surgery: a randomized controlled trial. Br. J. Anaesth. 2005. 95 (2). 183-8. doi: 10.1093/bja/aei172 [PubMed: 15951325]. 231.
- Murdoch H., Scrutton M., Laxton C.H. Choice of anaesthetic agents for caesarean section: a UK survey of current practice. Int. J. Obstet. Anesth. 2013. 22. 31-5.
- Myles P.S., Leslie K., McNeil J. et al. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet. 2004. 363. 1757-63.
- Oxford Textbook of Obstetric Anaesthesia. V. Clark, M. Van de Velde, R. Fernando. 1st ed. Oxford: University Press, 2016. 1072 p.
- Pandit J.J., Cook T.M. 5th National Audit Project of The –Royal College of Anaesthetists and the Association of Anaesthetists of Great Britain and Ireland. Accidental Awareness during General Anaesthesia in the United Kingdom and Ireland. Report and findings. London: The Royal College of Anaesthetists and the Association of Anaesthetists of Great Britain and Ireland, 2014. 270 p.
- Park J., Forrest J., Kolesar R. et al. Oral clonidine reduces postoperative PCA morphine requirements. Can. J. Anaesth. 1996. 43 (9). 900-906.
- Philipp M., Bred M., Hein L. Physiological significance of alpha(2)-adrenergic receptor sub type diversity: one receptor is not enough. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002. 283. 2. R 287-R 295.
- Polley L.S., Wong C.A. et al. Chestnut’s Obstetric Anesthesia: Principles and Practice. D.H. Chestnut, 5th ed. Philadelphia: Elsevier Inc., 2014. 1328 p.
- Pournajafian A., Rokhtabnak F., Kholdbarin A. et al. Comparison of remifentanil and fentanyl regarding hemodynamic changes due to endotracheal intubation in preeclamptic parturient candidate for Caesarean delivery. Anesth. Pain. 2012. 2. 90-3. 22.
- Reza F.M., Zahra F., Esmaeel F. et al. Preemptive analgesic effect of ketamine in patients undergoing elective cesarean section. Clin. J. Pain. 2010. 26. 3. 223-226.
- Robins K., Lyons G. Intraoperative awareness during general anesthesia for Caesarean delivery. Anesth. Analg. 2009. 109. 886-90.
- Rollins M., Lucero J. Overview of anesthetic considerations for Caesarean delivery. Br. Med. Bull. 2012. 101. 10525.
- Roofthooft E., Joshi G.P., Rawal N., Van de Velde M., PROSPECT Working Group of the European Society of Regional –Anaesthesia and Pain Therapy and supported by the Obstetric Anaes–thetists Association. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021 May. 76 (5). 665-680. doi: 10.1111/anae.15339.
- Safavi M., Honarmand A. Attenuation of cardiovascular responses to laryngoscopy and tracheal intubation. Middle. East. J. Anaesthesiol. 2008. 19. 1349-58. 20.
- Sanchez Munoz M.C., De Kock M., Forget P. What is the place of clonidine in anesthesia? Systematic review and meta-analyses of randomized controlled trials. Journal of Clinical Anesthesia. 2017. 38. 140-153. http://dx.doi.org/10.1016/j.jclinane.2017.02.003.
- Servey J., Chang J. Over-the-counter medications in pregnancy. Am. Fam. Physician. 2014. 90. 548-555.
- Shibli K.U., Russell I.F. A survey of anaesthetic techniques used for caesarean section in the UK in 1997. Int. J. Obstet. Anesth. 2000. 9. 3. 160-167.
- Soltanifar S., Russell R. The National Institute for Health and Clinical Excellence (NICE) guidelines for caesarean section, 2011 update: implications for the anaesthetist. Int. J. Obstet. Anesth. 2012. 21. 3. 264-272.
- Sumikura H., Niwa H., Sato M. Rethinking general anesthesia for cesarean section. J. Anesth. 2016. 30. 2. 268-273.
- The European Network of Teratology Information Servi–ces. ENTIS: Position statement on acetaminophen (paracetamol) in pregnancy. October 03, 2021. Available at: https://www.entis-org.eu/wp-content/uploads/2021/10/ENTIS-position-statement-on-acetami–nophen3.10.2021.pdf [Accessed: 14 October 2021].
- Treseng L., Brochet M., Ferreira E. Clonidine Use for the Treatment of Sialorrhea Gravidarum: A Case Series and Literature Review. Birth Defects Research Part A-Clinical and Molecular Teratology. Wiley-Blackwell 111 River St., Hoboken 07030–5774, NJ USA (2016).
- Turner R.J., Lambros M., Holmes C. Comparison of propofol and thiopentone for induction of anaesthesia for elective caesarean section. Anaesth. Intensive Care. 2002. 30. 5. 591-596.
- Westlund K.N., Carlton S.M., Zhang D. [et al.] Direct cate–cholaminergic innervation of primate spinothalamic tract neurons. J. Comp. Neurol. 1990. 299. 2. 178-86.
- WFSA. Update in Anaesthesia. Vol. 34. September 2019. P. 14-17.
- World health statistics 2015. World Health Organization. Geneva, 2015. Vol. 290. 161 p.
- Xie H.G., Cao Y.J., Gauda E.B. et al. Clonidine clearance matures rapidly during the early postnatal period: a population pharmacokinetic analysis in newborns with neonatal abstinence syndrome. J. Clin. Pharmacol. 2011. 51. 502-511.
- Yoo K.Y., Lee J.C., Yoon M.H. The effects of volatile anesthetics on spontaneous contractility of isolated human pregnant uterine muscle: a comparison among sevoflurane, desflurane, isoflurane, and halothane. Anesth. Analg. 2006. 103. 2. 443-444.