
Журнал «Медицина неотложных состояний» Том 19, №4, 2023
Вернуться к номеру
Порівняння ефективності найвіддаленіших підходів до аналгезії після тотальної артропластики кульшового суглоба
Авторы: Гавриков О.Є. (1, 2), Купін В.І. (2), Коломаченко В.І. (1, 2)
(1) — Харківський національний медичний університет, м. Харків, Україна
(2) — КНП ХОР «Обласна клінічна травматологічна лікарня», м. Харків, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
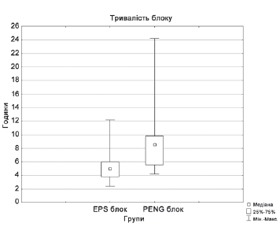
Актуальність. Останнім часом запропоновано два блоки, один з яких є найбільш проксимальним і зветься еrector spine plane (ESP) block; інший є найбільш дистальним і зветься pericapsular nerve group (PENG) block. Обидві методики виконуються під ультразвуковим контролем, позиціонуються як ефективні й безпечні, без м’язової слабкості. Мета роботи: оцінка клінічної ефективності найвіддаленіших підходів (ESP і PENG блоки) до знеболювання за адекватністю аналгезії та фізичною активністю пацієнтів після артропластики кульшового суглоба. Матеріали та методи. У дослідження було включено 70 пацієнтів ASA II–III, середній вік пацієнтів становив 64,6 ± 10,7 року, 40 жінок і 30 чоловіків, яким у плановому порядку було виконано первиннe тотальне ендопротезування кульшового суглоба з приводу захворювання або перелому під спінальною анестезією. Після операції в І групі (n = 35) виконували ESP блок, у ІІ групі (n = 35) — PENG блок, вводили 30 мл 0,25% розчину бупівакаїну. Оцінювалися здатність долати дистанцію 30 метрів без обмежень за часом, максимальна інтенсивність больового синдрому, потреба в опіоїдах (налбуфін), тривалість блоку і кількість пацієнтів з післяопераційними ускладненнями. Результати. Тривалість PENG блоку становила в середньому 8,6 (5,6–9,8) год, що статистично вірогідно перевищувало цей показник у пацієнтів, які отримали ESP блок — середня тривалість 5,0 (3,8–6,0) год (р < 0,001). При порівнянній аналгезії в обох групах пацієнтам, які отримали PENG блок, знадобилося для подолання 30-метрової дистанції менше часу після операції — 31,0 (27,0–47,0) год порівняно з тими, хто мав ESP блок, — 45,0 (32,0–54,0) год (р = 0,006). 28,6 % пацієнтів не потребували призначення опіоїдів у післяопераційному періоді в ІІ групі, а кількість таких пацієнтів у І групі становила лише 8,5 % (р = 0,036), що продемонструвало кращий аналгетичний потенціал PENG блоку. Висновки. З огляду на простоту виконання і безпечність обох регіонарних методик, а також ефективність PENG блок видається реальною альтернативою іншим регіонарним методикам у даної категорії пацієнтів.
Background. Recently, two blocks have been proposed: one of which is the most proximal and is called the erector spinae plane (ESP) block, the other is the most distal and is called pericapsular nerve group (PENG) block. Both techniques are performed under ultrasound control, are positioned as effective and safe, without muscle weakness. The purpose of the work: to evaluate the clinical effectiveness of the most remote approaches (ESP and PENG) for anesthesia in terms of the adequacy of analgesia and physical activity of patients after hip arthroplasty. Materials and methods. The study included 70 ASA II–III patients: 40 women and 30 men with an average age of 64.6 ± 10.7 years who underwent planned primary total hip arthroplasty for disease or fracture under spinal anesthesia. After the surgery, ESP block was performed in group I (n = 35), PENG block in group II (n = 35), 30 ml of 0.25% bupivacaine solution was injected. The ability to cover a distance of 30 meters without time limits, the maximum severity of the pain syndrome, the need for opioids (nalbuphine), the duration of the block and the number of patients with postoperative complications were evaluated. Results. The duration of PENG block was on average 8.6 (5.6–9.8) hours, which statistically significantly exceeded this indicator in patients who received ESP block with an average duration of 5 (3.8–6.0) hours (p < 0.001). With comparable analgesia in both groups, patients who received PENG block required less time to walk the 30-meter distance — 31.0 (27.0–47.0) hours compared to those who received ESP block — 45.0 (32.0–54.0) hours (p = 0.006). In group II, 28.6 % of patients did not need opioids in the postoperative period, and this indicator in group I was only 8.5 % (p = 0.036), demonstrating the better analgesic potential of PENG block. Conclusions. Given the ease of implementation and safety of both regional methods, as well as the effectiveness of PENG block, it appears to be a real alternative to other regional methods in this category of patients.
PENG блок; ESP блок; артропластика кульшового суглоба; регіонарна анестезія
PENG block; ESP block; total hip arthroplasty; regional anesthesia
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Maradit Kremers H., Larson D., Crowson C., Kremers W., Washington R., Steiner C. et al. Prevalence of Total Hip and Knee Replacement in the United States. The Journal of Bone and Joint Surgery-American. 2015. Vol. 97(17). 1386-1397. https://doi.org/10.2106/jbjs.n.01141.
- Johnson R., Kopp S., Burkle C., Duncan C., Jacob A., Erwin P. et al. Neuraxial vs general anaesthesia for total hip and total knee arthroplasty: a systematic review of comparative-effectiveness research. British Journal of Anaesthesia. 2016. 116(2). 163-176. https://doi.org/10.1093/bja/aev455.
- Greimel F., Maderbacher G., Zeman F., Grifka J., Meis-sner W., Benditz A. No Clinical Difference Comparing General, Regional, and Combination Anesthesia in Hip Arthroplasty: A Multicenter Cohort-Study Regarding Perioperative Pain Management and Patient Satisfaction. The Journal of Arthroplasty. 2017. 32(11). 3429-3433. https://doi.org/10.1016/j.arth.2017.05.038.
- Forero M., Adhikary S., Lopez H., Tsui C., Chin K. The Erector Spinae Plane Block. Regional Anesthesia and Pain Medicine. 2016. 41(5). 621-627. https://doi.org/10.1097/aap.0000000000000451.
- Singh S., Ranjan R., Lalin D. A new indication of erector spinae plane block for perioperative analgesia is total hip replacement surgery — A case report. Indian Journal of Anaesthesia. 2019. 63(4). 310. https://doi.org/10.4103/ija.ija_25_19.
- Tulgar S., Senturk O. Ultrasound guided Erector Spinae Plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. Journal of clinical anesthesia. 2018. 44. 68. https://doi.org/10.1016/j.jclinane.2017.11.006.
- Tsui B., Fonseca A., Munshey F., McFadyen G., Caruso T. The erector spinae plane (ESP) block: A pooled review of 242 cases. Journal of Clinical Anesthesia. 2019. 53. 29-34. https://doi.org/10.1016/j.jclinane.2018.09.036.
- Short A., Barnett J., Gofeld M., Baig E., Lam K., Agur A., Peng P. Anatomic Study of Innervation of the Anterior Hip Capsule. Regional Anesthesia and Pain Medicine. 2017. 1. https://doi.org/10.1097/aap.0000000000000701.
- Bugada D., Bellini V., Lorini L., Mariano E. Update on Selective Regional Analgesia for Hip Surgery Patients. Anesthesiology Clinics. 2018. 36(3). 403-415. https://doi.org/10.1016/j.anclin.2018.04.001.
- Del Buono R., Padua E., Pascarella G., Costa F., Tognù A., Terranova G. et al. Pericapsular nerve group block: an overview. Minerva Anestesiologica. 2021. 87(4). https://doi.org/10.23736/s0375-9393.20.14798-9.
- Morrison C., Brown B., Lin D., Jaarsma R., Kroon H. Anal-gesia and anesthesia using the pericapsular nerve group block in hip surgery and hip fracture: a scoping review. Regional Anesthesia & Pain Medicine. 2020. 46(2). 169-175. https://doi.org/10.1136/rapm-2020-101826.
- Tulgar S., Aydin M., Ahiskalioglu A., De Cassai A., Gurkan Y. Anesthetic Techniques: Focus on Lumbar Erector Spinae Plane Block. Local And Regional Anesthesia. 2020. Vol. 13. 121-133. https://doi.org/10.2147/lra.s233274.
- Elsharkawy H., Bajracharya G., El-Boghdadly K., Drake R., Mariano E. Comparing two posterior quadratus lumborum block approaches with low thoracic erector spinae plane block: an anatomic study. Regional Anesthesia & Pain Medicine. 2019. 44(5). 549-555. https://doi.org/10.1136/rapm-2018-100147.
- Girón-Arango L., Peng P., Chin K., Brull R., Perlas A. Pericapsular Nerve Group (PENG) Block for Hip Fracture. Regional Anesthesia and Pain Medicine. 2018. 1. https://doi.org/10.1097/aap.0000000000000847.
- Jakobsson J., Johnson M.Z. Perioperative regional anaesthesia and postoperative longer-term outcomes. F1000Research. 2016. 5. F1000 Faculty Rev-2501. https://doi.org/10.12688/f1000research.9100.1.
- Taketa Y., Irisawa Y., Fujitani T. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after video-assisted thoracic surgery: a randomized controlled non-inferiority clinical trial. Regional Anesthesia & Pain Medicine. 2019. 45(1). 10-15. https://doi.org/10.1136/rapm-2019-100827.
- Tulgar S., Selvi O., Senturk O., Ermis M., Cubuk R., Ozer Z. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. Journal of Clinical Anesthesia. 2018. 47. 5-6. https://doi.org/10.1016/j.jclinane.2018.02.014.
- Celik M., Tulgar S., Ahiskalioglu A., Alper F. Is high volume lumbar erector spinae plane block an alternative to transforaminal epidural injection? Evaluation with MRI. Regional anesthesia and pain medicine. Advance online publication. 2019. https://doi.org/10.1136/rapm-2019-100514.
- Tulgar S., Kose H. C., Selvi O., Senturk O., Thomas D.T., Ermis M.N., Ozer Z. Comparison of Ultrasound-Guided Lumbar Erector Spinae Plane Block and Transmuscular Quadratus Lumborum Block for Postoperative Analgesia in Hip and Proximal Femur Surgery: A Prospective Randomized Feasibility Study. Anesthesia, essays and researches. 2018. 12(4). 825-831. https://doi.org/10.4103/aer.AER_142_18.
- Mysore K., Sancheti S., Howells S., Ballah E., Sutton J., Uppal V. Postoperative analgesia with pericapsular nerve group (PENG) block for primary total hip arthroplasty: a retrospective study. Canadian Journal of Anesthesia/Journal Canadien D’anesthésie. 2020. 67(11). 1673-1674. https://doi.org/10.1007/s12630-020-01751-z.
- Siddiqui Z., Cepeda S., Denman W., Schumann R., Carr D. Continuous Lumbar Plexus Block Provides Improved Analgesia With Fewer Side Effects Compared With Systemic Opioids After Hip Arthroplasty. Regional Anesthesia And Pain Medicine. 2007. 32(5). 393-398. doi: 10.1097/00115550-200709000-00006.
- Wiesmann T., Steinfeldt T., Wagner G., Wulf H., Schmitt J., Zoremba M. Supplemental single shot femoral nerve block for total hip arthroplasty: impact on early postoperative care, pain management and lung function. Minerva Anestesiologica. 2014. 80(1). 48-57.
- Desmet M., Vermeylen K., Van Herreweghe I., Carlier L., Soetens F., Lambrecht S., Croes K., Pottel H., Van de Velde M. A Longitudinal Supra-Inguinal Fascia Iliaca Compartment Block Reduces Morphine Consumption after Total Hip Arthroplasty. Regional anesthesia and pain medicine. 2017. 42(3). 327-333. https://doi.org/10.1097/AAP.0000000000000543.
- Selvi O., Tulgar S. Ultrasound guided erector spinae plane block as a cause of unintended motor block. Bloqueo en el plano del erector de la columna ecoguiado como causa de bloqueo motor imprevisto. Revista espanola de anestesiologia y reanimacion. 2018. 65(10). 589-592. https://doi.org/10.1016/j.redar.2018.05.009.
- De Cassai A., Fasolo A., Geraldini F., Munari M. Motor block following bilateral ESP block. Journal of Clinical Anesthesia. 2020. 60. 23. https://doi.org/10.1016/j.jclinane.2019.08.029.
- Karaca O., Pinar H.U. Is high dose lumbar erector spinae plane block safe? Journal of clinical anesthesia. 2020. 62. 109721. https://doi.org/10.1016/j.jclinane.2020.109721.