
Журнал «Медицина неотложных состояний» Том 19, №5, 2023
Вернуться к номеру
Рівень С-реактивного протеїну у хворих на гостру тромбоемболію легеневої артерії
Авторы: Целуйко В.Й. (1), Курінна М.В. (1, 2), Яковлева Л.М. (1)
(1) — Харківський національний університет імені В.Н. Каразіна, м. Харків, Україна
(2) — КНП «Міська клінічна лікарня № 8» Харківської міської ради, м. Харків, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
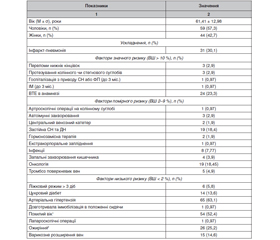
Актуальність. Сучасна стратифікація ризику хворих на тромбоемболію легеневої артерії (ТЕЛА) не враховує всіх можливих чинників, які можуть впливати на перебіг та прогноз захворювання. З огляду на це перспективним є дослідження маркерів запального процесу, насамперед С-реактивного протеїну (СРП), щодо їх прогностичної цінності при ТЕЛА. Метою дослідження було вивчення клінічного та прогностичного значення підвищення рівня СРП у хворих на ТЕЛА у госпітальний період. Матеріали та методи. Обстежено 103 пацієнти з підтвердженим на МСКТ-ангіографії легеневої артерії (ЛА) або на секції діагнозом «гостра ТЕЛА», яким був визначений СРП при госпіталізації. Крім загальноклінічного обстеження, у всіх хворих оцінювали фактори ризику ТЕЛА та ризик ранньої смерті згідно з рекомендаціями ESC-2019. Лабораторне обстеження крім основних досліджень включало кількісне визначення КФК-МВ, D-димеру та СРП. Серед інструментальних досліджень проводились електрокардіографія, ехокардіографія та МСКТ-ангіографія ЛА. Результати. Залежно від рівня СРП хворі були поділені на дві групи за медіаною цього показника, яка становила 26 мг/л. У групу 1 (СРП < 26 мг/л) увійшли 52 хворі, у групу 2 (СРП > 26 мг/л) — 51 хворий. Встановлено, що в групі 1 переважала частка пацієнтів низького ризику (р = 0,044) та середнє значення балів за PESI було вірогідно нижчим (р = 0,011). У групі 2 було вірогідно нижче середнє значення сатурації кисню в крові (SpO2) при госпіталізації (р = 0,004), вірогідно більшими були середні значення розмірів лівого шлуночка (ЛШ) — КДР та КСР (р = 0,045 та р = 0,043 відповідно) та вірогідно нижчою — фракція викиду (ФВ) ЛШ (р = 0,002); крім того, у групі 2 вірогідно вищими були середні рівні лейкоцитів (р = 0,0003), нейтрофілів (р = 0,00001), ШОЕ (р = 0,012), сечовини (р = 0,008) та КФК-МВ (р = 0,028). При проведенні кореляційного аналізу виявлений вірогідний зворотний зв’язок між рівнями СРП та вихідним рівнем SpO2 та прямий зв’язок між рівнем СРП та розміром правого передсердя (ПП), рівнем КФК-МВ та зростанням ризику ранньої смертності від ТЕЛА. Висновки. У 92 % хворих з гострою ТЕЛА відзначалось підвищення рівня СРП, вищий рівень якого був асоційований з вірогідним зниженням SpO2 (р < 0,004), збільшенням розмірів ЛШ (р < 0,05) та зменшенням ФВ (р < 0,003). За результатами кореляційного аналізу доведений зв’язок між рівнем СРП та ризиком за шкалою PESI, SpO2, рівнем КФК-МВ та розміром ПП.
Background. Modern risk stratification in patients with pulmonary embolism (PE) does not consider all possible factors that may influence the course and prognosis of the disease. In view of this, it is promising to study inflammatory markers, especially C-reactive protein (CRP), for their prognostic value in PE. The purpose was to study the clinical and prognostic value of increased CRP levels in patients with PE during hospitalization. Material and methods. One hundred and three patients with diagnosis of acute PE confirmed by computed tomographic pulmonary angiography (CTPA) or by autopsy were examined, their СRP level was evaluated during hospitalization. In addition to a general clinical examination, all patients were screened for PE risk factors and risk of premature death according to the ESC 2019 guidelines. La-boratory tests included quantitative determination of CPK-MB, D-dimer and СRP in addition to basic ones. Electrocardiography, echocardiography, and CTPA were performed as part of the instrumental studies. Results. Depending on the СRP median (26 mg/l), patients were divided into two groups. Group 1 (СRP < 26 mg/l) included 52 people, group 2 (СRP > 26 mg/l) — 51 patients. It was found that in group 1, patients with low risk predominated (p = 0.044) and the average pulmonary embolism severity index was significantly lower (p = 0.011). In group 2, the average blood oxygen saturation (SpO2) during hospitalization was significantly lower (p = 0.004), the average parameters of the left ventricle, namely end-diastolic and end-systolic volume, were significantly greater (p = 0.045 and p = 0.043, respectively), and the ejection fraction was significantly lower (p = 0.002). Also, the average levels of leukocytes (p = 0.0003), neutrophils (p = 0.00001), urea (p = 0.008), CPK-MB (p = 0.028) and erythrocyte sedimentation rate (p = 0.012) were significantly higher in group 2. Correlation analysis revealed a reliable inverse connection between CRP levels and initial SpO2 and a direct relationship between CRP level and the size of the right atrium, CPK-MB level, and increased risk of early mortality from PE. Conclusions. Elevated CRP was found in 92 % of patients with acute PE and was associated with a significant decrease in SpO2 (p < 0.004), increased left ventricular size (p < 0.05), and decreased ejection fraction (p < 0.003). Correlation analysis revealed a relationship between CRP level and the risk according to the pulmonary embolism severity index, SpO2, the level of CPK-MB and the size of the left atrium.
тромбоемболія легеневої артерії, С-реактивний протеїн, ехокардіографія, МСКТ-ангіографія ЛА
pulmonary embolism; C-reactive protein; echocardio-graphy; computed tomographic pulmonary angiography
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Tseluyko V.Y., Yakovleva L.M., Sukhova S.M., Radchenko O.V. Factors related to the improvement of the right ventricular function in patients with pulmonary embolism at short-term follow-up. Emergency Medicine. 2022. 18(1). 42-47. doi: 10.22141/2224-0586.18.1.2022.1457.
- Tseluyko V.Y., Yakovleva L.M., Sukhova S.M., Kinoshenko K.Y., Radchenko O.V., Vnukova A.S. Clinical and anamnestic characteristics and risk factors in patients with acute pulmonary embolism among residents of Kharkiv. Emergency Medicine. 2021. 17(3). 58-63. doi: 10.22141/2224-0586.17.3.2021.234810.
- Turetz M., Sideris A.T., Friedman O.A., Triphathi N., Horo-witz J.M. Epidemiology, Pathophysiology, and Natural History of Pulmonary Embolism. Semin. Intervent. Radiol. 2018. 35(2). 92-98. doi: 10.1055/s-0038-1642036.
- Konstantinides S.V., Meyer G., Becattini C., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020. 41(4). 543-603. doi: 10.1093/eurheartj/ehz405.
- Wändell P., Forslund T., Danin Mankowitz H., et al. Venous thromboembolism 2011–2018 in Stockholm: a demographic study. J. Thromb. Thrombolysis. 2019. 48(4). 668-673. doi: 10.1007/s11239-019-01966-y.
- Aghajani H., Hashemi S., Karimi A., Yadangi S., Jalali A., Jenab Y. Predictors and mortality of patients with delayed pulmonary embolism diagnosis: A cohort study. Caspian J. Intern. Med. 2022. 13(4). 757-764. doi: 10.22088/cjim.13.4.757.
- Heit J.A., Spencer F.A., White R.H. The epidemiology of venous thromboembolism. J. Thromb. Thrombolysis. 2016. 41(1). 3-14. doi: 10.1007/s11239-015-1311-6.
- Parkhomenko O.M., Lutai Y.M. Venous thromboembolism: modern approaches to the diagnosis of pulmonary embolism. Cardiolo-gy, Rheumatology, Cardiac Surgery. 2020. 6. 15-17. https://health-ua.com/article/63695-venoznij-tromboembolzm-suchasn-pdhodi-dodagnost iki-tromboembol-legenevo-art.
- Piovella F., Iosub D.I. Acute pulmonary embolism: risk assessment, risk stratification and treatment options. The Clinical Respiratory Journal. 2016. 10(5). 545-554. doi: 10.1111/crj.12264.
- Hepburn-Brown M., Darvall J., Hammerschlag G. Acute pulmonary embolism: a concise review of diagnosis and management: A review of acute pulmonary embolism. Intern. Med. J. 2019. 49(1). 15-27. doi: 10.1111/imj.14145.
- Cuomo J.R., Arora V., Wilkins T. Management of Acute Pulmonary Embolism With a Pulmonary Embolism Response Team. J. Am. Board Fam. Med. 2021. 34(2). 402-408. doi: 10.3122/jabfm.2021.02.200308.
- Saghazadeh A., Hafizi S., Rezaei N. Inflammation in venous thromboembolism: Cause or consequence? Int. Immunopharmacol. 2015. 28(1). 655-665. doi: 10.1016/j.intimp.2015.07.044.
- Folsom A.R., Lutsey P.L., Heckbert S.R., et al. Longitudinal increase in blood biomarkers of inflammation or cardiovascular disease and the incidence of venous thromboembolism. J. Thromb. Haemost. 2018. 16(10). 1964-1972. doi: 10.1111/jth.14241.
- Branchford B.R., Carpenter S.L. The Role of Inflammation in Venous Thromboembolism. Frontiers in Pediatrics. 2018. 6. Accessed May 14, 2023. https://www.frontiersin.org/articles/10.3389/fped.2018.00142.
- Vazquez-Garza E., Jerjes-Sanchez C., Navarrete A., Joya-Harrison J., Rodriguez D. Venous thromboembolism: thrombosis, inflammation, and immunothrombosis for clinicians. J. Thromb. Thrombolysis. 2017. 44(3). 377-385. doi: 10.1007/s11239-017-1528-7.
- Dix C., Zeller J., Stevens H., et al. C-reactive protein, immunothrombosis and venous thromboembolism. Frontiers in Immuno-logy. 2022. 13. Accessed May 16, 2023. https://www.frontiersin.org/articles/10.3389/fimmu.2022.1002652.
- Gewurz H. Biology of C-reactive protein and the acute phase response. Hosp. Pract. (Hosp. Ed). 1982. 17(6). 67-81. doi: 10.1080/21548331.1982.11702332.
- Galeano-Valle F., Ordieres-Ortega L., Oblitas C.M., Del-Toro-Cervera J., Alvarez-Sala-Walther L., Demelo-Rodríguez P. Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review. Int. J. Mol. Sci. 2021. 22(5). 2627. doi: 10.3390/ijms22052627.
- Yousuf M., Reza S., Zafar S., et al. Role of Serum Markers in Combination as a Diagnostic Tool for Acute Pulmonary Embolism: Cross-Sectional Study. Cureus. 2020. 12(9). e10584. doi: 10.7759/cureus.10584.
- Gok M., Kurtul A. A novel marker for predicting severity of acute pulmonary embolism: systemic immune-inflammation index. Scandinavian Cardiovascular Journal. 2021. 55(2). 91-96. doi: 10.1080/14017431.2020.1846774.
- Omar H.R., Mirsaeidi M., Rashad R., et al. Association of Serum Albumin and Severity of Pulmonary Embolism. Medicina (Kaunas). 2020. 56(1). 26. doi: 10.3390/medicina56010026.
- Peng R., Yin W., Wang F., et al. Neutrophil levels upon admission for the assessment of acute pulmonary embolism with intermediate- and high-risk: an indicator of thrombosis and inflammation. Thromb J. 2023. 21(1). 28. doi: 10.1186/s12959-023-00471-w.
- Büyükşirin M., Anar C., Polat G., Karadeniz G. Can the Level of CRP in Acute Pulmonary Embolism Determine Early Mortality? Turk Thorac. J. 2021. 22(1). 4-10. doi: 10.5152/TurkThoracJ.2020.19048.
- Verma S., Yeh E.T.H. C-reactive protein and atherothrombosis-beyond a biomarker: an actual partaker of lesion formation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003. 285(5). R1253-1256; discussion R1257-1258. doi: 10.1152/ajpregu.00170.2003.
- Ohigashi H., Haraguchi G., Yoshikawa S., et al. Comparison of biomarkers for predicting disease severity and long-term respiratory prognosis in patients with acute pulmonary embolism. Int. Heart J. 2010. 51(6). 416-420. doi: 10.1536/ihj.51.416.
- Lippi G., Favaloro E.J., Montagnana M., Franchini M. C-reactive protein and venous thromboembolism: causal or casual association? Clin. Chem. Lab. Med. 2010. 48(12). 1693-1701. doi: 10.1515/CCLM.2010.335.
- Abul Y., Karakurt S., Ozben B., Toprak A., Celikel T. C-reactive protein in acute pulmonary embolism. J. Investig. Med. 2011. 59(1). 8-14. doi: 10.2310/jim.0b013e31820017f2.
- Karadeniz G., Çil E. What are the mortality markers in elderly patients with acute pulmonary embolism? Eur. Rev. Med. Pharmacol. Sci. 2023. 27(1). 159-165. doi: 10.26355/eurrev_202301_30867.
- Ammari Z., Hasnie A.A., Ruzieh M., et al. Prognostic Value of Computed Tomography Versus Echocardiography Derived Right to Left Ventricular Diameter Ratio in Acute Pulmonary Embolism. Am. J. Med. Sci. 2021. 361(4). 445-450. doi: 10.1016/j.amjms.2020.07.008.