
Журнал «Медицина неотложных состояний» Том 19, №5, 2023
Вернуться к номеру
Менеджмент артеріальної гіпотензії після спінальної анестезії під час кесаревого розтину: багатоцентрове опитування лікарів та огляд літератури
Авторы: Титаренко Н.В., Вознюк А.В., Дацюк О.І., Сливка Е.В., Літвінов С.К., Костюченко А.В., Мазур Г.М., Сергійчук О.В., Бевз Г.В.
Вінницький національний медичний університет ім. М.І. Пирогова, м. Вінниця, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
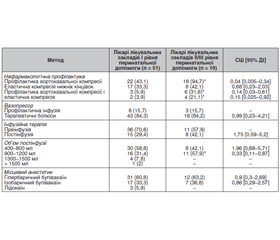
Актуальність. Артеріальна гіпотензія під час кесаревого розтину в умовах спінальної анестезії виникає в 75–90 % випадків і може викликати побічні ефекти з боку матері й новонародженого. Мета дослідження: проаналізувати дотримання анестезіологами рекомендацій чинних протоколів з менеджменту артеріальної гіпотензії під час спінальної анестезії в пологових стаціонарах/відділеннях м. Вінниці та Вінницької області. Матеріали та методи. Проведено багатоцентрове опитування, у якому взяли участь 70 лікарів-анестезіологів із 21 пологового стаціонару/відділення лікувальних закладів м. Вінниці та Вінницької області. Електронний опитувальник включав запитання щодо заходів профілактики й лікування артеріальної гіпотензії під час кесаревого розтину в умовах спінальної анестезії. Результати. 98,5 % із 70 анестезіологів, які надають допомогу акушерським пацієнтам у м. Вінниці та Вінницькій області, рутинно використовують фенілефрин для підтримання гемодинаміки після спінальної анестезії. Однак частка респондентів, які використовують вазопресор профілактично, становить лише 15,7 %. Встановлено, що на додаток до фенілефрину лікарі здійснюють нефармакологічну профілактику гіпотензії після спінальної анестезїі: 35,7 % — профілактику аортокавальної компресії, 8,5 і 12,9 % — еластичну компресію нижніх кінцівок з профілактикою аортокавальної компресії або без неї відповідно, а також більшість (67,1 %) анестезіологів призначають преінфузію як кристалоїдами, так і колоїдами, а подальший об’єм постінфузії кристалоїдів становить від 400 до 1500 мл і більше. Найбільш часто для спінальної анестезії анестезіологи Вінниччини використовують гіпербаричний бупівакаїн (60 %), рідше — ізобаричний бупівакаїн (35,7 %) і лідокаїн (4,3 %). Висновки. Аналіз поточної практики свідчить про необхідність розробки й упровадження чіткої єдиної стратегії менеджменту артеріальної гіпотензії з вазопресорами при кесаревому розтині під спінальною анестезією в рамках програми прискореного відновлення породіль у м. Вінниці та Вінницькій області.
Background. Hypotension during caesarean section under spinal anesthesia occurs in 75–90 % of cases and may causes adverse effects in a mother and newborn. The purpose of the work is to analyze the adherence of anesthesiologists to the guidelines of current protocols on the management of hypotension during spinal anesthesia in maternity hospitals/departments of Vinnytsia and Vinnytsia region. Materials and methods. We conducted a multicenter survey involving 70 anesthesiologists from 21 maternity hospitals or departments of medical facilities in Vinnytsia and Vinnytsia region. Our electronic questionnaire included questions about measures to prevent and treat hypotension during cesarean section under spinal anesthesia. Results. 98.5 % of 70 anesthesiologists who provide care for the obstetric patients in Vinnytsia and Vinnytsia region routinely use phenylephrine to maintain hemodynamics after spinal anesthesia. However, the share of respondents who use a vasopressor prophylactically is only 15.7 %. It was found that, in addition to phenylephrine, doctors perform non-pharmacological prevention of hypotension after spinal anesthesia: 35.7 % — prevention of aortocaval compression, 8.5 and 12.9 % — elastic compression of the lower extremities with/without prevention of aortocaval compression, respectively. Also, most anesthesiologists (67.1 %) prescribe pre-infusion with both crystalloids and colloids and the subsequent post-infusion volume of crystalloid solutions is 400 to 1500 ml or more. According to the data obtained, anesthesiologists in Vinnytsia region most often use hyperbaric bupivacaine (60 %); isobaric bupivacaine (35.7 %) and lidocaine (4.3 %) for spinal anesthesia are used less often. Conclusions. The analysis of current practice indicates the need to develop and implement a clear unified strategy for managing hypotension with vasopressors during caesarean section under spinal anesthesia within the framework of the program of accelerated recovery of women in labor in Vinnytsia and Vinnytsia region.
кесарів розтин; спінальна анестезія; артеріальна гіпотензія; інфузія; вазопресори
cesarean section; spinal anesthesia; hypotension; infusion; vasopressors
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Lei Yang, Xu Cheng, Di Yang et al. General versus Neuraxial Anesthesia in Cesarean Section: A Systematic Review. J. Anesth. Perioper. Med. 2017. № 4. Р. 114-122.
- Roofthooft E., Joshi G.P., Rawal N. et al. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021. № 76(5). Р. 665-680.
- Nag D.S., Samaddar D.P., Chatterjee A. et al. Vasopressors in obstetric anesthesia: a current perspective. World J. Clin. Cases. 2015. № 3(1). Р. 58-64.
- Sharwood-Smith G., Drummond G.B. Hypotension in obstetric spinal anaesthesia: a lesson from pre-eclampsia. Br. J. Anaesth. 2009. № 102(3). Р. 291-294.
- Lim G., Facco F.L., Nathan N. et al. A review of the impact of obstetric anesthesia on maternal and neonatal outcomes. Anesthesiology. 2018. № 129(1). Р. 192-215.
- Pattinson R. Saving Mothers 2011–2013: The Sixth Report of the National Committee for Confidential Enquiries into Maternal Deaths in South Africa [Internet]. Pretoria: Government Printer; 2019. 91 р. http://www.kznhealth.gov.za/mcwh/ Maternal/Saving-Mothers-2011-2013-short-report.pdf.
- Klöhr S., Roth R., Hofmann T. et al. Definitions of hypotension after spinal anaesthesia for caesarean section: literature search and application to parturients. Acta Anaesthesiol. Scand. 2010. № 54(8). Р. 909-921.
- Kinsella S.M., Carvalho B., Dyer R.A. et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia. 2018. № 73(1). Р. 71-92.
- Bollag L., Lim G., Sultan P. et al. Society for Obstetric Anesthesia and Perinatology: Consensus Statement and Recommendations for Enhanced Recovery After Cesarean. Anesth. Analg. 2021. № 132(5). Р. 1362-1377.
- Caesarean birth NICE guideline. Published: 31 March 2021. www.nice.org.uk/guidance/ng192.
- Practice guidelines for obstetric anesthesia: An updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology. 2016. № 124(2). Р. 270-300.
- Наказ МОЗ України «Про затвердження Уніфікованого клінічного протоколу первинної, вторинної (спеціалізованої) та третинної (високоспеціалізованої) медичної допомоги «Кесарів розтин» № 8 від 05.01.2022. https://www.dec.gov.ua/wp-content/uploads/2022/01/2022_08_ykpmd_kesar_roztyn.pdf.
- Бевз Г.В., Титаренко Н.В. Вибір методу знеболювання кесарева розтину у роділей Вінницької області. Здоровье женщины. 2015. № 10 (106). С. 101-103.
- Farber M.K., Bateman B.T. Phenylephrine Infusion: Driving a Wedge in Our Practice of Left Uterine Displacement? Anesthesiology. 2017. № 127(2). Р. 212-214.
- Rees S.G., Thurlow J.A., Gardner I.C. et al. Maternal cardiovascular consequences of positioning after spinal anaesthesia for Caesarean section: left 15 degree table tilt vs. left lateral. Anaesthesia. 2002. № 57(1). Р. 15-20.
- Lee A., Landau R., Mattingly J.L. et al. Left lateral table tilt for elective caesarean delivery under spinal anesthesia has no effect on neonatal acid-base status. Anesthesiology. 2017. № 127(2). Р. 241-249.
- Cluver C., Novikova N., Hofmeyr G.J. et al. Maternal position during caesarean section for preventing maternal and neonatal complications. Cochrane Database Syst. Rev. 2013. (3). CD007623.
- Cyna A., Andrew M., Emmett R. et al. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database of Syst. Rev. 2006. 4. CD002251.
- Burns S.M., Cowan C.M., Wilkes R.G. Prevention and managment of hypotension during spinal anaesthesia for elective Caesarean section: a survey of practice. Anaesthesia. 2001. № 56(8). Р. 777-798.
- Ngan Kee W.D., Khaw K.S., Tan P.E. et al. Placental transfer and fetal metabolic effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. Anesthesiology. 2009. № 111(3). Р. 506-512.
- Fitzgerald J.P., Fedoruk K.A., Jadin S.M. et al. Prevention of hypotension after spinal anaesthesia for caesarean section: a systematic review and network meta-analysis of randomised controlled trials. Anaesthesia. 2020. № 75(1). Р. 109-121.
- Heesen M., Rijs K., Hilber N. et al. Ephedrine versus phenylephrine as a vasopressor for spinal anaesthesia-induced hypotension in parturients undergoing high-risk caesarean section: meta-analysis, meta-regression and trial sequential analysis. Int. J. Obstet. Anesth. 2019. № 37. Р. 16-28.
- McDonnell N.J., Paech M.J., Muchatuta N.A. et al. A randomised double-blind trial of phenylephrine and metaraminol infusions for prevention of hypotension during spinal and combined spinal-epidural anaesthesia for elective caesarean section. Anaesthesia. 2017. № 72(5). Р. 609-617.
- Siddik-Sayyid S.M., Taha S.K., Kanazi G.E. et al. A randomized controlled trial of variable rate phenylephrine infusion with rescue phenylephrine boluses versus rescue boluses alone on physician interventions during spinal anesthesia for elective cesarean delivery. Anesthesia and Analgesia. 2014. № 118(3). Р. 611-618.
- Jackson R., Reid J.A., Thorburn J. Volume preloading is not essential to prevent spinal-induced hypotension at caesarean section. Br. J. Anaesth. 1995. № 75(3). Р. 262-265.
- Powell M., Mathru M., Brandon A. et al. Assessment of endothelial glycocalyx disruption in term parturients receiving a fluid bolus before spinal anesthesia: a prospective observational study. Int. J. Obstet. Anesth. 2016. № 28. Р. 100.
- Banerjee A., Stocche R.M., Angle P. et al. Preload or coload for spinal anesthesia for elective Cesarean delivery: a meta-analysis. Can. J. Anaesth. 2010. № 57(1). P. 24-31. doi: 10.1007/s12630-009-9206-7.
- McDonald S., Fernando R., Ashpole K. et al. Maternal cardiac output changes after crystalloid or colloid coload following spinal anesthesia for elective cesarean delivery: a randomized controlled trial. Anesth. Analg. 2011. № 113(4). Р. 803-810.
- Chan V.W., Peng P., Chinyanga H. et al. Determining minimum effective anesthetic concentration of hyperbaric bupivacaine for spinal anesthesia. Anesth. Analg. 2000. № 90(5). Р. 1135-1140.
- Sng B.L., Han N.L.R., Leong W.L. et al. Hyperbaric vs. isobaric bupivacaine for spinal anaesthesia for elective caesarean section: a Cochrane systematic review. Anaesthesia. 2018. № 73(4). Р. 499-511.
- Weiniger C.F., Heesen M., Knigin D. et al. Association Between Hyperbaric Bupivacaine Dose and Maternal Hypotension: Retrospective Database Study of 8226 Women Undergoing Cesarean Delivery Under Spinal Anesthesia. Anesth. Analg. 2021. № 133(4). Р. 967-975.
- Lee J., George R.B., Habib A.S. Spinal induced hypotension: incidence, mechanisms, prophylaxis and management: summarizing 20 years of research. Best Pract. Res. Clin. Anaesthesiol. 2017. № 31(1). Р. 57-68.