
Международный эндокринологический журнал Том 19, №6, 2023
Вернуться к номеру
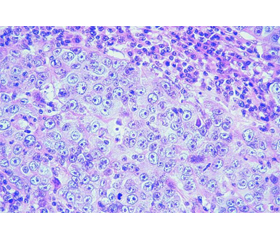
Рідкісний випадок медулярної карциноми
Авторы: Ліщук О.З., Суслик Г.І., Урбанович А.М.
Львівський національний медичний університет імені Данила Галицького, м. Львів, Україна
Рубрики: Эндокринология
Разделы: Справочник специалиста
Версия для печати
На частку медулярного раку щитоподібної залози (МРЩЗ) припадає 5–10 % від усіх випадків раку щитоподібної залози. Більшість випадків (75 %) мають спорадичний характер, однак частка пацієнтів з МРЩЗ і синдромом сімейної схильності є найвищою серед хворих з будь-яким синдромом спадкового раку (близько 25 %), і цю можливість слід ураховувати при оцінці пацієнта з МРЩЗ. До сімейних синдромів належать множинна ендокринна неоплазія (MEН) 2A, MEН 2B і сімейний не-MEН МРЩЗ (сімейний МРЩЗ). Сімейні синдроми МРЩЗ трапляються приблизно в одному випадку на 30 тис. населення. Знижена пенетрантність і клінічна мінливість є загальновизнаними особливостями багатьох моногенних розладів, зокрема фенотипів, пов’язаних з RET-протоонкогеном. Вони потребують індивідуальної оцінки патогенних ефектів і клінічного значення будь-якої ідентифікованої нової послідовності RET-варіанта як передумови індивідуального генетичного консультування і планування медичного спостереження і лікування. Висвітлено діагностичні критерії захворювання, розглянуто молекулярно-генетичні аспекти, визначено тактику лікування і подальшого спостереження. У статті описаний клінічний випадок рідкісного варіанта МРЩЗ. Розглядається лікування даної патології з проведенням радикальної екстрафасціальної тиреоїдектомії. З огляду на неефективність радіойод- і хіміотерапії основним завданням у лікуванні МРЩЗ є рання діагностика, радикальне хірургічне втручання, активний моніторинг з метою раннього виявлення рецидиву хвороби. При плануванні профілактичної тиреоїдектомії рекомендовано орієнтуватися на стратифікацію рівня мутацій гена RET і терміни проведення профілактичної тиреоїдектомії, запропоновані Американською тиреоїдною асоціацією. Упровадження в клінічну практику молекулярно-генетичного дослідження з метою діагностики МРЩЗ дає змогу об’єктивізувати генетичну лінію захворювання в біологічної родини. Своєчасно встановлений діагноз МРЩЗ дає змогу призначити адекватне лікування на етапі доклінічних проявів захворювання, що може значно поліпшити якість і тривалість життя.
Medullary thyroid cancer (MTC) accounts for 5–10 % of all thyroid cancers. Most cases (75 %) are sporadic, but the proportion of patients with MTC and a familial predisposition syndrome is the highest among those with any hereditary cancer syndrome (about 25 %), and this possibility should be considered when examining a patient with MTC. Familial syndromes include multiple endocrine neoplasia (MEN) 2A, MEN 2B, and non-MEN familial MTC (familial MTC). Familial MTC syndromes occur in approximately one case per 30,000 of the population. Reduced penetrance and clinical variability are well-established features of many monogenic disorders, particularly phenotypes associated with the RET proto-oncogene. They require an individual assessment of the pathogenic effects and clinical significance of any identified new sequence of the RET variant as prerequisites for individual genetic counseling and planning of medical monitoring and treatment. Diagnostic criteria for the disease have been outlined, molecular and genetic aspects have been discussed, and the determination of treatment and further observation has been addressed. The article describes a clinical case of a rare variant of MTC. Treatment of this pathology with radical extrafascial thyroidectomy is under consideration. Given the ineffectiveness of radioiodine and chemotherapy, the main task in the treatment of MTC is early diagnosis, radical surgical intervention, and active monitoring aimed at early detection of disease recurrence. When planning prophylactic thyroidectomy, it is recommended to focus on the stratification of the level of RET gene mutations and the timing of prophylactic thyroidectomy proposed by the American Thyroid Association. The introduction of molecular genetic research into clinical practice for the purpose of diagnosing MTC allows for the objective assessment of the genetic lineage of the disease within a biological family. A timely diagnosis of MTC makes it possible to prescribe an adequate treatment at the stage of preclinical manifestations of the disease, which can significantly increase the quality and duration of life.
медулярна карцинома; кальцитонін; щитоподібна залоза; RET-протоонкоген
medullary carcinoma; calcitonin; thyroid gland; RET proto-oncogene
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Censi S., Manso J., Mian C. Other markers of medullary thyroid cancer, not only calcitonin. Eur. J. Endocrinol. 2023 Jan 10. 188(1). lvac009. doi: 10.1093/ejendo/lvac009. PMID: 36651167.
- Verbeek H.H.G., B de Groot J.W., Sluiter J.W. et al. Calcitonin testing for detection of medullary thyroid cancer in people with thyroid nodules. Cochrane Systematic Review Diagnostic Version published: 2020. https://doi.org/10.1002/14651858.CD010159.pub2.
- Tiedje V., Ting S., Dralle H., Schmid K.W., Fuhrer D. Medul–lary thyroid carcinoma. Internist (Berl.). 2015. 56. 1019-31. (in German).
- Wells S.A. Jr, Asa S.L., Dralle H. et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015. 25. 567-610. doi: 10.1089/thy.2014.0335.
- Filetti S., Durante C., Hartl D., Leboulleux S., Locati L.D., Newbold K., Papotti M.G., Berruti A.; ESMO Guidelines Committee. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019 Dec 1. 30(12). 1856-1883. doi: 10.1093/annonc/mdz400. PMID: 31549998.
- Viola D., Elisei R. Management of Medullary Thyroid Cancer. Endocrinol. Metab. Clin. North Am. 2019 Mar. 48(1). 285-301. doi: 10.1016/j.ecl.2018.11.006. Epub 2018 Dec 26. PMID: 30717909.
- Raue F., Frank-Raue K. Long-Term Follow-up in Medullary Thyroid Carcinoma. Recent Results Cancer Res. 2015. 204. 207-25. doi: 10.1007/978-3-319-22542-5_10. PMID: 26494391.
- Qi X.P., Lin G.B., Chen B., Li F., Cao Z.L., Zheng W.H., Zhao J.Q. Multiple Endocrine Neoplasia Type 2B Associated Mixed Medullary and Follicular Thyroid Carcinoma in A Chinese Patient with RET M918T Germline Mutation. Endocr. Metab. Immune Disord. Drug Targets. 2021. 21(3). 554-560. doi: 10.2174/1871530320666200713092633. PMID: 32660411.
- Fugazzola L. Medullary thyroid cancer — An update. Best Pract. Res. Clin. Endocrinol. Metab. 2023 Jan. 37(1). 101655. doi: 10.1016/j.beem.2022.101655. Epub 2022 Mar 31. PMID: 35422397.
- Thomas C.M., Asa S.L., Ezzat S., Sawka A.M., Goldstein D. Diagnosis and pathologic characteristics of medullary thyroid carcinoma-review of current guidelines. Curr. Oncol. 2019 Oct. 26(5). 338-344. doi: 10.3747/co.26.5539. Epub 2019 Oct 1. PMID: 31708652; PMCID: PMC6821118.
- Woliński K., Kaznowski J., Klimowicz A., Maciejewski A., Łapińska-Cwojdzińska D., Gurgul E. et al. Diagnostic value of selec–ted biochemical markers in the detection of recurrence of medullary thyroid cancer — comparison of calcitonin, procalcitonin, chromo–granin A, and carcinoembryonic antigen. Endokrynol. Pol. 2017. 68(4). 434-437. doi: 10.5603/EP.a2017.0038. Epub 2017 Jun 6. PMID: 28585679.
- Trimboli P., Mian C., Piccardo A., Treglia G. Diagnostic tests for medullary thyroid carcinoma: an umbrella review. Endocrine. 2023 Aug. 81(2). 183-193. doi: 10.1007/s12020-023-03326-6. Epub 2023 Mar 6. PMID: 36877452; PMCID: PMC10293444.
- Trimboli P., Guidobaldi L., Bongiovanni M., Crescenzi A., Alevizaki M., Giovanella L. Use of fine-needle aspirate calcitonin to detect medullary thyroid carcinoma: A systematic review. Diagn. Cytopathol. 2016 Jan. 44(1). 45-51. doi: 10.1002/dc.23375. Epub 2015 Oct 19. PMID: 26481456.
- Leimbach R.D., Hoang T.D., Shakir M.K.M. Diagnostic Challenges of Medullary Thyroid Carcinoma. Oncology. 2021. 99(7). 422-432. doi: 10.1159/000515373. Epub 2021 Apr 20. PMID: 33878761.
- Kebebew E., Ituarte P.H., Siperstein A.E., Duh Q.Y., Clark O.H. Medullary thyroid carcinoma: clinical characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer. 2000 Mar 1. 88(5). 1139-48. doi: 10.1002/(sici)1097-0142(20000301)88:5<1139::aid-cncr26>3.0.co;2-z. PMID: 10699905.
- Skinner M.A., Moley J.A., Dilley W.G., Owzar K., Debe–nedetti M.K., Wells S.A. Jr. Prophylactic thyroidectomy in multiple endocrine neoplasia type 2A. N. Engl. J. Med. 2005 Sep 15. 353(11). 1105-13. doi: 10.1056/NEJMoa043999. PMID: 16162881.
- Palamarchuk V.O., Voytenko V.V., Shapoval N.O., Ogryzko T.V. A clinical case of a familial form of medullary thyroid cancer. Clinical endocrinology and endocrine surgery. 2021. 1(73). 76-81. doi: 10.30978/CEES-2021-1-76 (in Ukrainian).