
Международный эндокринологический журнал Том 21, №1, 2025
Вернуться к номеру
Upstreаm-терапія реперфузійних порушень гемодинаміки, ритму і провідності у хворих на гострий інфаркт міокарда, що розвинувся на тлі цукрового діабету та метаболічного синдрому (друге повідомлення)
Авторы: Швед М.І., Ястремська І.О., Овсійчук Р.М., Мартинюк Л.П., Прокопович О.А., Кіцак Я.М.
Тернопільський національний медичний університет імені І.Я. Горбачевського, м. Тернопіль, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
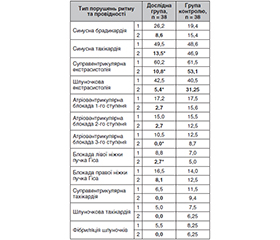
Актуальність. У літературі недостатньо даних щодо механізмів впливу цукрового діабету 2-го типу (ЦД2) та метаболічного синдрому (МС) на частоту розвитку ускладнень у хворих на інфаркт міокарда (ІМ), а також не розроблено ефективних методів їх корекції. Мета роботи: оцінити частоту розвитку реперфузійних ускладнень та ефективність upstream-терапії у хворих на гострий інфаркт міокарда в поєднанні з ЦД2 та МС шляхом включення в програму терапії курсу L-карнітину/L-аргініну та інгібітору НЗКТГ-2 дапагліфлозину. Матеріали та методи. Обстежено 38 хворих на гострий коронарний синдром (ГКС (STEMI)) на тлі ЦД2 та МС (основна дослідна група) та 38 хворих на ГКС (STEMI) без ЦД2 і МС (група порівняння). Окрім загальноклінічних методів, проводили детальне лабораторне та інструментальне обстеження: біохімічний аналіз крові, визначення рівнів глюкози, інсуліну, індексу HOMA-IR, ліпідограми, коагулограми, креатинфосфокінази (КФК-МВ), тропоніну Т, ЕКГ, трансторакальну ехокардіографію (ЕхоКГ) та коронарну ангіографію (КАГ). Ризик внутрішньогоспітальної летальності прогнозували за шкалою GRACE. Усім пацієнтам з ГКС (STEMI) проведено ургентну КАГ з подальшою балонною ангіопластикою та стентуванням інфаркт-залежної вінцевої артерії, а також проводили стандартну медикаментозну терапію згідно з чинним протоколом МОЗ та додатково призначали хворим дослідної групи дапагліфлозин по 10 мг/добу і 5 внутрішньовенних вливань L-аргінін-L-карнітинової суміші (відповідно 4,2 та 2,0 г) в 100 мл розчинника. Результати. На ГКС (STEMI) на тлі ЦД2 та МС вірогідно частіше хворіють чоловіки середнього віку. Розвиток STEMI асоціювався з наявністю коморбідних станів: артеріальної гіпертензії, ЦД2 та МС, хронічної хвороби нирок та комбінованих факторів ризику ІХС. Тяжкість клінічного стану хворих була зумовлена гострою серцевою недостатністю (ГСН) ІІІ–ІV ст. та наявністю таких життєзагрозливих ускладнень гострого періоду ІМ, як шлуночкові порушення ритму (у 45,3 %) та провідності (у 23,8 %), набряк легень (у 17,3 %), гостра аневризма лівого шлуночка (у 13,3 %). Компенсація вуглеводного обміну у коморбідних хворих на ІМ у поєднанні з ЦД2 та МС за допомогою дапагліфлозину супроводжувалась вірогідним зниженням частоти життєзагрозливих ускладнень ІМ: частота порушень ритму у хворих дослідної групи знизилася з 87,5 до 50,0 %, ГСН за Killip II–ІІІ ФК — з 70,0 до 12,5 %, що було вірогідно порівняно з групою контролю. Додавання до складу протокольної програми терапії курсу парентерального застосування L-аргініну (4,2 г/д) та L-карнітину (2,0 г/д) сприяло зменшенню постінфарктного ремоделювання серця та зростанню фракції викиду (на 7 %). У такій ситуації цитопротекторна терапія на фоні лікування інгібітором НЗКТГ-2 дапагліфлозином виступає як патогенетична upstreаm-терапія. Висновки. У хворих з ГКС (STEMI) на тлі ЦД2 та МС у вихідному стані спостерігаються гіперглікемія, інсулінорезистентність та виражені порушення морфофункціональних параметрів серця з його систолічно-діастолічною дисфункцією, які є тригерами ускладненого перебігу цієї патології, з розвитком синдрому серцевої недостатності та порушень ритму і провідності. Застосування комплексного лікування з включенням L-карнітину та L-аргініну на фоні терапії інгібітором SGLT2 дапагліфлозином як upstreаm-терапії сприяє відновленню чутливості тканин до інсуліну, поліпшенню вуглеводневого обміну, приводить до поліпшення параметрів центральної кардіогемодинаміки, що супроводжується вірогідним зменшенням частоти розвитку та вираженості гострої лівошлуночкової недостатності та життєзагрозливих реперфузійних аритмій.
Background. There is a lack of scientific data on the mechanisms of influence of type 2 diabetes mellitus (T2DM) and metabolic syndrome (MS) on the incidence of complications in patients with myocardial infarction; no effective methods of their correction have been developed. The purpose of the study was to evaluate the incidence of reperfusion complications and the effectiveness of upstream therapy in patients with acute myocardial infarction combined with T2DM and MS by including L-carnitine/L-arginine and dapagliflozin, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, in the treatment program. Materials and methods. We examined 38 patients with acute ST-elevation myocardial infarction (STEMI) on the background of T2DM and MS (study group) and 38 patients with STEMI without T2DM and MS (control group). In addition to the use of general clinical methods, detailed laboratory and instrumental examinations were performed: biochemical blood tests, evaluation of glucose, insulin, HOMA-IR, lipidogram, coagulogram, creatine kinase-MB, troponin T, electrocardiography, transthoracic echocardiography and coronary angiography. The risk of in-hospital mortality was predicted by the GRACE score. All patients with STEMI underwent urgent coronary angiography with subsequent balloon angioplasty and the infarct-dependent internal carotid artery stenting, as well as standard drug therapy according to the Ministry of Health protocol and were additionally prescribed dapagliflozin 10 mg/day and 5 intravenous infusions of L-arginine-L-carnitine mixture (4.2 and 2.0 g, respectively) in 100 ml of solvent. Results. STEMI on the background of T2DM and MS is significantly more common in middle-aged men. The development of STEMI was associated with the presence of comorbid conditions: hypertension, T2DM and MS, chronic kidney disease, and combined risk factors for coronary heart disease. The severity of the patient’s clinical condition was due to congestive heart failure III–IV and the presence of life-threatening complications of the acute period of myocardial infarction such as ventricular arrhythmias (45.3 %), conduction disorders (23.8 %), pulmonary edema (17.3 %), and acute left ventricular aneurysm (13.3 %). Compensation of carbohydrate metabolism in patients with myocardial infarction combined with T2DM and MS using dapagliflozin was accompanied by a significant reduction in the incidence of life-threatening complications: the incidence of rhythm disturbances in patients of the study group decreased from 87.5 to 50.0 %, heart failure (Killip class II–III) — from 70.0 to 12.5 %, which was significant compared with the control group. The inclusion of parenteral arginine (4.2 g/day) and L-carnitine (2.0 g/day) in the protocol therapy program contributed to a decrease in postinfarction cardiac remodeling and an increase in ejection fraction by 7 %. In this situation, cytoprotective therapy against the background of treatment with the SGLT2 inhibitor dapagliflozin acts as a pathogenetic upstream therapy. Conclusions. In patients with STEMI combined with T2DM and MS, hyperglycemia, insulin resistance and severe abnormalities of morphological and functional parameters of the heart with its systolic-diastolic dysfunction are observed at baseline, which are triggers of the complicated course of this pathology, with the development of heart failure syndrome, rhythm and conduction disorders. The comprehensive treatment with the inclusion of L-carnitine and L-arginine against the background of using the SGLT2 inhibitor dapagliflozin as upstream therapy helps restore tissue sensitivity to insulin, improve carbohydrate metabolism, central cardiovascular hemodynamics that is accompanied by a significant reduction in the frequency and severity of acute left ventricular failure and life-threatening reperfusion arrhythmias.
гострий коронарний синдром; цукровий діабет; метаболічний синдром; інсулінорезистентність; серцева недостатність; аритмії та блокади; L-карнітин/L-аргінін; інгібітор SGLT2 дапагліфлозин
acute coronary syndrome; diabetes mellitus; metabolic syndrome; insulin resistance; heart failure; arrhythmias and blocks; L-carnitine/L-arginine; SGLT2 inhibitor dapagliflozin
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ivanyuk АV, Orlova NM. Ischemic heart disease among the population of working age in Kyiv region: statistical analysis of the modern epidemiological situation. Reports of Vinnytsia National Me–dical University. 2020;24(4):694-9. doi: https://doi.org/10.31393/reports-vnmedical-2020-24(4)-24.
- Gach O, El HZ, Lancellotti P. Acute coronary syndrome. Rev Med Liege. 2018 May;73(5-6):243-250. In French. PMID: 29926562.
- Сіренко Ю.М. Стан проблеми серцево-судинної захворюваності та смертності в Україні. Ліки України. 2022. 2(258). 11-14. https://doi.org/10.37987/1997-9894.2022.2(258).264084.
- Shved M, Yastremska I, Kuchmiy V, Ovsiychuk R. ST-elevation myocardial infarction in patients with type 2 diabetes mellitus. Influence of the SGLT2 inhibitor dapagliflozin. International Journal оf Endocrinology (Ukraine). 2024;20(1):11-17. https://doi.org/10.22141/2224-0721.20.1.2024.1352.
- Daryabor G, Atashzar MR, Kabelitz D, Meri S, Kalantar K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front Immunol. 2020;11:1582. doi: 10.3389/fimmu.2020.01582.
- Petrie JR, Guzik TJ, Touyz RM. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mecha–nisms. Can J Cardiol. 2018 May;34(5):575-584. doi: 10.1016/j.cjca.2017.12.005.
- Shved M, Yastremska I, Ovsiichuk R. Correction of changes in lipid metabolism and redox system in patients with STEMI in the setting of insulin resistance. Scientific and Practical Journal. 2023 Apr. 12 [cited 2025 Jan. 18];25(1):77-82. DOI: 10.21802/artm.2023.1.25.77.
- Daryabor G, Kabelitz D, Kalantar K. An update on immune dysregulation in obesity-related insulin resistance. Scand J Immunol. 2019;89:12747. DOI: 10.1111/sji.12747.
- Fahed M, Abou Jaoudeh MG, Merhi S, Mosleh JMB, Gha–dieh R, Al Hayek S, El Hayek Fares JE. Evaluation of risk factors for insulin resistance: a cross sectional study among employees at a private university in Lebanon. BMC Endocr Disord. 2020 Jun 10;20(1):85. doi: 10.1186/s12902-020-00558-9.
- Chia CW, Egan JM, Ferrucci L. Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circ Res. 2018 Sep 14;123(7):886-904. doi: 10.1161/CIRCRESAHA.118.312806.
- Okadome Y, Morinaga J, Fukami H, Hori K, Ito T, Sato M, et al. Hyperglycemia and Thrombocytopenia — Combinatorially Increase the Risk of Mortality in Patients with Acute Myocardial Infarction Undergoing Veno-Arterial Extracorporeal Membrane Oxygenation. Circ Rep. 2021 Oct 27;3(12):707-715. doi: 10.1253/circrep.
- Shved MI, Yastremska IO, Martynyuk LP, Yastremska SO, Dobrianskyi TO. Management of central hemodynamic and endothelial function disturbances in patients with myocardial infarction combined with metabolic syndrome. Pol Merkur Lekarski. 2021 Oct 22;49(293):325-328. PMID: 34800016.
- Koval SM, Yushko KO, Snihurska IO, Starchenko TG, Pankiv VI, Lytvynova OM, Mysnychenko OV. Relations of angiotensin-(1-7) with hemodynamic and cardiac structural and functional parameters in patients with hypertension and type 2 diabetes. Arterial Hypertension. 2019;23(3):183-189. DOI: 10.5603/AH.a2019.0012.
- Zheng J, Cheng J, Wang T, Zhang Q, Xiao X. Does HbA1c Level Have Clinical Implications in Diabetic Patients Undergoing Coro–nary Artery Bypass Grafting? A Systematic Review and Meta-Analysis. Int J Endocrinol. 2017;2017:1537213. doi: 10.1155/2017/1537213.
- Chen Y, Zhang H, Hou X, Li X, Qian X, Feng X, et al. Glycemic control and risk factors for in-hospital mortality and vascular complications after coronary artery bypass grafting in patients with and without preexisting diabetes. J Diabetes. 2021 Mar;13(3):232-242. doi: 10.1111/1753-0407.13108.
- Pankiv V. Glucocentric and cardiocentric approaches to achieving type 2 diabetes compensation. International Journal оf Endocrinology (Ukraine). 2023;19(5):344-348. https://doi.org/–10.22141/2224-0721.19.5.2023.1297.
- Li S, Vandvik PO, Lytvyn L, et al. SGLT-2 inhibitors or GLP-1 receptor agonists for adults with type 2 diabetes: a clinical practice guideline [published correction appears in BMJ. 2022 Apr 28;377:o1080]. BMJ. 2021;373:n1091. doi: 10.1136/bmj.n1091.
- Mantsiou C, Karagiannis T, Kakotrichi P, et al. Glucagon-like peptide-1 receptor agonists and sodium-glucose co-transporter-2 inhi–bitors as combination therapy for type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes Metab. 2020;22(10):1857-1868. doi: 10.1111/dom.14108\.
- Posch MG, Walther N, Ferrannini E, et al. Metabolic, Intestinal, and Cardiovascular Effects of Sotagliflozin Compared with Empagliflozin in Patients With Type 2 Diabetes: A Randomized, Double-Blind Study. Diabetes Care. 2022;45(9):2118-2126. doi: 10.2337/dc21-2166.
- Inzucchi SE, Khunti K, Fitchett DH, Wanner C, Mattheus M, George JT, et al. Cardiovascular Benefit of Empagliflozin Across the Spectrum of Cardiovascular Risk Factor Control in the EMPA-REG OUTCOME Trial. J Clin Endocrinol Metab. 2020 Sep 1;105(9):3025-35. doi: 10.1210/clinem/dgaa321.
- Nessler J. Dapagliflozin in the treatment of patients with heart failure with reduced left ventricular ejection fraction — practical approach. Postepy Kardiol Interwencyjnej. 2021 Jun;17(2):135-140. doi: 10.5114/aic.2021.107491.
- Das US, Paul A, Banerjee S. SGLT2 inhibitors in heart failure with reduced ejection fraction. Egypt Heart J. 2021 Oct 24;73(1):93. doi: 10.1186/s43044-021-00218-w.
- Unified Clinical Protocol for emergency, primary, secondary (specialized), tertiary (highly specialized) medical care and cardiac rehabilitation “Acute coronary syndrome with ST segment elevation”. September 4, 2021, Order of the Ministry of Health of Ukraine No. 1936.
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. doi: 10.1093/eurheartj/ehx393.
- Gonskyi YaI. Biological chemistry: Laboratory practice. Ternopil: Ukrmedknyga. 2001. 288.
- American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Echocardiography; American Heart Association; ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardio–graphy. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardio–graphy, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. J Am Soc Echocardiogr. 2011;24(3):229-267. doi: 10.1016/j.echo.2010.12.008.
- Shved M, Dobrianskyi T, Yastremska I, Heriak S, Liakhovych R, Kitsak Ya, Kyrychok I. Treatment-Induced Changes in the Quality of Life of Patients with Myocardial Infarction Combined with Comorbid Critical Ischemia of Lower Extremities. Journal of International Dental and Medical Research. 2022;15(3):1113-1121.
- GUSTO investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med. 1993 Sep 2;329(10):673-82. doi: 10.1056/NEJM199309023291001. PMID: 8204123.
- DiNicolantonio JJ, Lavie CJ, Fares H, Menezes AR, O’Keefe JH. L-carnitine in the secondary prevention of cardiovascular di–sease: systematic review and meta-analysis. Mayo Clin Proc. 2013 Jun;88(6):544-51. doi: 10.1016/j.mayocp.2013.02.007. Epub 2013 Apr 15. PMID: 23597877.
- Shved M, Yastremska I, Levytska L, Kuchmiy V, Proko–povych O, Kitsak Y, Liakhovych R. Clinical portrait of a patient with acute coronary syndrome and type 2 diabetes mellitus: a novel stra–tegy for the diagnosis, prognosis and treatment. International Journal оf Endocrinology (Ukraine). 2024;20(7):504-510. https://doi.org/–10.22141/2224-0721.20.7.2024.1449.
- Wang ZY, Liu YY, Liu GH, Lu HB, Mao CY. L-Carnitine and heart disease. Life Sci. 2018 Feb 1;194:88-97. doi: 10.1016/j.lfs.2017.12.015. Epub 2017 Dec 11. PMID: 29241711.
- Colonna P, Iliceto S. Myocardial infarction and left ventri–cular remodeling: results of the CEDIM trial. Carnitine Ecocardiografia Digitalizzata Infarto Miocardico. Am Heart J. 2000 Feb;139(2 Pt 3):S124-30. doi: 10.1067/mhj.2000.103918. PMID: 10650326.
- George J, Shmuel SB, Roth A, Herz I, Izraelov S, Deutsch V, et al. L-arginine attenuates lymphocyte activation and anti-oxidized LDL antibody levels in patients undergoing angioplasty. Atherosclerosis. 2004 Jun;174(2):323-7. doi: 10.1016/j.atherosclerosis.2004.01.025. PMID: 15136062.