
Международный эндокринологический журнал 5 (69) 2015
Вернуться к номеру
Endogenous peptide apelin and pathological cardiac remodeling in hypertension patients with type 2 diabetes
Авторы: Koval S., Iushko K., Starchenko T. - GI "L.T.Malaya Therapy National Institute of the NAMS of Ukraine“, Kharkiv, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
Introduction. Type 2 diabetes mellitus (T2DM) in 2-2.5 times more common in patients with arterial hypertension than in normotensive patients. The combination of these diseases increases the risk of cardiovascular complications in several times. Pathological cardiac remodeling and its dysfunction is inherent in patients with hypertension, accelerated by combination with T2DM, including the development of left ventricular (LV) hypertrophy, increasing the left atrium (LA) size and the development of diastolic dysfunction. Concentric LV hypertrophy at the same time is one of the strongest predictors of increased cardiovascular risk. Therefore it is important searches and exploring new pathogenetic factors that influence the progression of both arterial hypertension and T2DM and involved in the development of heart damage.
Apelin is a mediator of cardiovascular control, which is involved in the development of arterial hypertension, coronary heart disease, atherosclerosis, heart failure, arrhythmias. However, apelin influences on carbohydrate metabolism, increases glucose utilization, reduces insulin resistance. But the data of the role of apelin in the processes of pathological cardiac remodeling in arterial hypertension with T2DM are limited.
The purpose of the study was to investigate the level apelin in hypertension patients with T2DM and determine its relationship with structural and functional parameters of the heart and types of pathological cardiac remodeling.
Material and methods. The study involved 63 hypertension patients grade 2-3 in combination with T2DM aged 40 to 70 years. The men were 32 patients (51%), women – 31 people (49%). The mean duration of arterial hypertension in patients was (14.6±1.1) years and of T2DM was (5.25±0.75) years. The mild form of T2DM was observed in 11 individuals (17.46%), moderate severity – in 52 patients (82.54%). In 13 patients (20.63%) T2DM was first established.
Cardiac parameters were studied using echocardiography in B and M modes by the standard method. LV mass (LVM) was calculated by the Devereux method (1986). For the upper limit of normal LVM index considered the 110 g/cm2 for women and 125 g/cm2 for men. To identify different types of LV hypertrophy used the method A.Ganau (1992), which was isolated by 4 types of structural and geometric LV changes: normal geometry, concentric remodeling, concentric hypertrophy and eccentric hypertrophy. LV diastolic function was assessed according to the Doppler transmitral inflow pattern.
Apelin blood levels were determined using ELISA kits «Phoenix Pharmaceuticals Inc.».
The control group consisted of 16 healthy individuals.
Statistical data processing was performed using the software package Statistica for Windows, version 6.0.
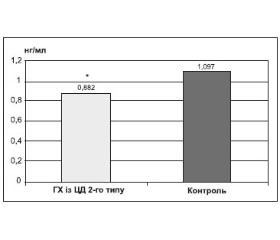
Results. The blood concentration of apelin in hypertensive patients with T2D was significantly lower than in healthy individuals. Thus, the level of apelin in hypertension patients with T2DM was 0.882 (0.788; 0.924) ng/ml versus 1.097 (0.944; 1.171) ng/ml of the control group, p <0.001.
The results Kruskel-Wallis test was shown significant influence of apelin blood levels on LVM, LVM index, relative wall thickness (RWT), interventricular septal wall thickness (SWT), posterior wall thickness (PWT), LA size and the type of cardiac geometry in hypertension patients with T2DM. Correlation analysis showed significant negative correlation of apelin levels with SWT (r=-0,50, p<0,001), PWT (r=-0,46, p<0,001), LVM (r=-0,39, p <0,01), LVM index (r=-0,42, p<0,001), LA size (r=-0,45, p<0,001).
Depending on left ventricular remodeling the lowest apelin levels observed in concentric LV hypertrophy – 0,855(0.722; 0.899) ng/ml. Apelin blood levels at all types of pathological cardiac remodeling was significantly lower than in control group and in patients with concentric LV hypertrophy the investigational peptide was significantly lower than in patients with LV concentric remodeling, p<0.05.
The blood levels of apelin significantly positively correlated with the E/A ratio (r=0.38, p<0.05) and the deceleration time (DT) (r=0.31, p<0.05) have been found. Concentration of apelin in hypertension patients with T2DM and diastolic dysfunction was 0.865 (0.750; 0.903) ng/ml and it was significantly lower than among patients with normal diastolic function of the heart (0.932 (0.892; 0.964) ng/ml) and control group (p<0.01 and p<0.001 respectively).
Conclusions. In hypertension patients with T2DM compared to healthy subjects determined significant decreasing of apelin blood levels. Reduced levels of apelin are associated with development of pathological cardiac remodeling primarily concentric LV hypertrophy. Negative correlation of apelin with major cardiac structural parameters that characterize the pathological cardiac ventricular remodeling (LVM, LVM index, RWT, SWT, PWT) and the LA size have been found. In patients with LV diastolic dysfunction observed decreasing of apelin blood levels compared with patients with normal diastolic function. Discovered reduction of the apelin blood levels and it correlation with the parameters of pathological cardiac remodeling and diastolic dysfunction may point to a significant role of deficiency of apelin in the progression of hypertension and diabetic heart damage in arterial hypertension on a background of T2DM.